One of the problems with a mishap involving an aircraft without a full suite of flight data recorders is that much of the evidence is destroyed by the impact of the crash and the fire that follows. That is the case with many accidents caused by slow onset hypoxia.
— James Albright
Updated:
2015-07-11
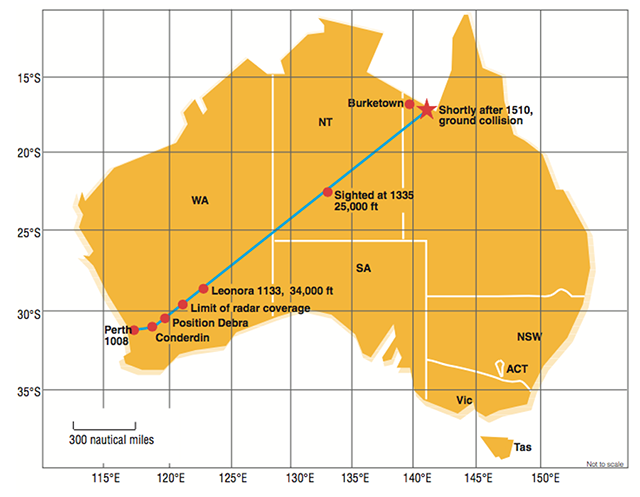
Investigation Report, figure 1.
Regardless, there are many lessons to be learned:
- Fuselage pressure leaks should be addressed immediately and repaired.
- Oxygen supply and delivery equipment must be pre-flighted.
- During every climb, part of your 10,000 foot check must be a check of cabin altitude. Most airplanes have a maximum cabin altitude between 6,000 and 8,000 feet. You certainly should not be above that at 10,000 feet aircraft altitude. You should know your normal cabin climb rate, typically around 300 fpm. Even if it takes you ten minutes to get to 10,000 feet aircraft altitude, you should not see more than 3,000 feet cabin altitude at that point. In any case, if it isn't where it should be, level off and investigate.
- When troubleshooting a pressurization problem, donning oxygen quickly will not only improve your mental capabilities, it can keep you in the game if things go south quickly or insidiously.
- When in doubt, descend.
1
Accident report
- Date: 4 Sep 2000
- Time: 1510 UTC
- Type: Beechcraft 200 Super King Air
- Operator: Central Air
- Registration: VH-SKC
- Fatalities: 1 of 1 crew, 7 of 7 passengers
- Aircraft Fate: Destroyed
- Phase: En route
- Airports: (Departure) Perth Airport, WA (PER/YPPH), Australia
- Airports: (Destination) Leonora Airport, WA (LNO/YLEO), Australia
2
Narrative
- On 4 September 2000, a Beech Super King Air 200 aircraft, VH-SKC, departed Perth, Western Australia at 1009 UTC (1809 Western Standard Time) on a charter flight to Leonora, with one pilot and seven passengers on board. The passengers were employees of a mining company returning to duty at the mine. After takeoff, the aircraft tracked as instructed by the air traffic services (ATS) controller. At 1010, the pilot was cleared to climb to flight level (FL)130, an altitude of approximately 13,000 ft.
- At 1015, as the aircraft climbed through 7,500 ft, the controller asked the pilot if the aircraft could reach FL160 by 36 NM from Perth. The pilot replied in the affirmative, and the controller cleared him to climb to FL 250, the planned cruising level, with the requirement to reach FL160 by 36 NM from Perth.
- At 1020, as the aircraft passed through FL156, the controller cleared the pilot to fly direct to position DEBRA, which was on the Cunderdin to Leonora track. The pilot correctly acknowledged the transmission, and flew the aircraft to DEBRA.
- At about 1033, as the aircraft climbed through FL 256, the controller requested the pilot to verify the aircraft’s altitude. The pilot replied, “Sierra Kilo Charlie–um–standby.”
- The ATC radar display showed that the aircraft’s altitude continued to increase.
- Over the period from 1034 to 1043, eight open microphone transmissions were made from the aircraft, the longest being about 4 minutes. The ATS Automatic Voice Recorder (AVR) recording of those transmissions contained the following:
- one unintelligible syllable;
- sounds of a person breathing;
- two chime-like tones, similar to those generated by electronic devices; and
- background noise that was consistent with engine/propeller noise.
- There were no detectable sounds on the recording that indicated passenger activity, such as moving, coughing or talking.
- The pilot did not answer further radio transmissions made by the controller to the aircraft. Requests by the controller for the pilot to select the IDENT function on the aircraft’s transponder (“squawk ident”) and to change frequency did not produce any response.
- The King Air continued to climb on the DEBRA to Leonora track and at 1102, the aircraft left radar coverage 218 NM (404 km) northeast of Perth while it was climbing through an altitude of FL 325. At 1133, at the request of Australian Search and Rescue (AusSAR), the crew of a business jet aircraft flew near the King Air for a short period, while it was near Leonora. The jet crew reported that the King Air was maintaining FL 343 on a steady heading of about 050 ̊M. Although the King Air’s external navigation and strobe lights were on, the jet crew saw no lights or movements inside the aircraft. The jet crew reported that the brightness of the strobe lights in the night conditions made it difficult to see inside the King Air.
- At 1335, the King Air was sighted northwest of Alice Springs by the crews of two other aircraft that had been tasked to intercept and follow it. The King Air was passing FL 250 in a steady descent, maintaining a heading of approximately 050 ̊M. The two chase aircraft remained with the King Air for the remainder of its flight. The crews reported that as the rate of the descent of the King Air slowly increased, its air speed increased to more than 200 kts. Although its external lights were on, nothing could be seen inside the cabin. The crews of the chase aircraft attempted to contact the pilot of the King Air by radio but they did not receive a response.
- At 1510, the crew of one chase aircraft observed the King Air, at an altitude of less than 5,000 ft, turn left through 90 ̊. The King Air then impacted the ground and caught fire about 65 km southeast of Burketown. The aircraft disintegrated on impact. There were no survivors.
Source: Investigation Report, ¶1.1
3
Analysis
- Civil Aviation Order (CAO) 108.26, Issue 1 (current at the time of the occurrence), Paragraph 3.1 stated: "An oxygen system for an aircraft which is intended for operations at flight altitudes above 25,000 feet shall include a device to provide the flight crew with a warning whenever the cabin pressure altitude exceeds 10,000 feet. Note: The cabin pressure warning should not depend on the reading of the gauge. An aural warning is strongly recommended.
- Occurrences ATSB 199902928 and ATSB 200105188, illustrated how pilots, occupied with other tasks, have missed visual warnings. Studies have shown that warning systems in complex domains such as aviation and medicine were made more effective by supplementing the systems’ visual indications with aural warnings.
- A warning annunciator panel located in the cockpit contained ten red warning annunciator lights, which indicated faults that required immediate action by the pilot. The ALT WARN annunciator illuminated whenever the cabin altitude exceeded 12,500 ft. The illumination of any red warning annunciator also triggered a red, flashing MASTER WARNING light on the glareshield in front of each pilot seat. The flashing MASTER WARNING light could be extinguished by pressing the lens cover on either of the lights. Extinguishing the MASTER WARNING flasher did not extinguish the warning annunciator that triggered it. Removing the condition or defect, which caused the annunciator to illuminate, was required.
- The aircraft was fitted with three devices that produced aural warning tones. They were:
- an altitude alerting device that sounded a chime and illuminated a light when the aircraft was 1,000 ft before the selected altitude. Another chime was sounded and light illuminated anytime the aircraft deviated 200 ft or more from the selected altitude;
- a buzzer that sounded continuously whenever the aircraft’s angle of attack exceeded a preset value indicating that an aerodynamic stall was imminent; and
- a horn that sounded intermittently whenever the landing gear was not locked down, in combination with various power lever and flap positions.
- The aircraft was not fitted with a high cabin altitude aural warning device, nor was it required to be.
Source: Investigation Report, ¶1.6
- There was nothing found during the examination of the aircraft’s bleed air system components that indicated any pre-existing problem that would have affected their operation at the time of the accident.
- The oxygen bottle was empty and its regulating valve was loose. Fire and impact forces damaged both. A crew oxygen mask connection socket and mask connector were recovered in the fully coupled state indicating that the mask assembly was connected to the aircraft at the time of impact. All the passenger oxygen mask containers had separated from the roof of the cabin during the impact sequence or had been destroyed in the fire. The oxygen system pressure gauge from the cockpit was destroyed by fire.
- No evidence was found to suggest that the oxygen system was unserviceable at the time of impact. Due to the extreme damage to the aircraft, it was not possible to determine:
- the quantity, if any, of oxygen in the system at the time of impact;
- the positions of the oxygen system controls prior to impact;
- whether the passenger oxygen masks deployed or had been used during the flight; or
- whether either of the two crew masks had been used during the flight.
- It was not possible to determine whether any ruptures in the pressure hull were present before impact, because the fuselage broke up during the impact sequence and was damaged by the post-impact fire.
Source: Investigation Report, ¶1.12
- The lack of evidence supporting the presence of toxic fumes and the speech and breathing symptoms displayed by the pilot during the radio transmissions associated with the observed lack of movement within the aircraft, indicated that the occupants were probably incapacitated by hypoxia. The occupants were probably incapacitated by hypobaric hypoxia as a result of inadequate cabin pressurisation.
Source: Investigation Report, ¶2.3
- The lack of pressurisation was due to insufficient air flowing into the cabin and/or as a result of air flowing from the cabin that exceeded the capacity of the pressurisation system. These conditions could have been a result of someone making an in appropriate switch selection (such as the occurrence reported in ATSB report 199902928) or due to a mechanical failure. Due to the lack of evidence, the investigation could not determine whether the depressurisation was a result of human error or mechanical failure.
- During an explosive or rapid depressurisation of a pressurised aircraft, however, the noise, pressure changes, temperature changes and draughts within the cabin would have alerted the occupants that a substantial failure had occurred. The considerable noise resulting from a rapid or explosive depressurisation would have likely produced a noise signature detectable in AVR recordings. In the absence of such a noise signature, the investigation concluded that a rapid or explosive depressurisation probably did not occur.
Source: Investigation Report, ¶2.4
- As hypobaric hypoxia took effect, the pilot’s visual acuity and colour discrimination would have reduced, making the red warning lights even less likely to be noticed by the pilot. An aural warning was more likely to have been detected and acted upon by the pilot than a visual warning alone. An aural warning for high cabin altitude may also have gained the pilot’s attention when the cabin altitude exceeded 10,000 ft, well before he may have experienced significant effects of hypoxia. Had the visual warning system been set to provide the warning when the cabin pressure altitude exceeded 10,000 feet rather than 12,500 feet, and functioned normally, the pilot would have had more time to observe and react to the warning.
Source: Investigation Report, ¶2.6
4
Cause
- After the aircraft climbed above the assigned altitude of FL 250, the speech and breathing patterns of the pilot, evidenced during the radio transmissions, displayed changes consistent with hypoxia.
- The incapacitation of the pilot and passengers was probably due to hypobaric hypoxia because of the high cabin altitude and their not receiving supplemental oxygen.
- The reasons for the pilot and passengers not receiving supplemental oxygen could not be determined.
- Setting the visual alert to operate when the cabin pressure altitude exceeds 10,000 ft and incorporating an aural warning in conjunction with the visual alert, may have prevented the accident.
- The aircraft was probably unpressurised for a significant part of its climb and cruise for undetermined reasons.
- The pilot and passengers were incapacitated, probably due to hypobaric hypoxia, because of the high cabin altitude and their not receiving supplemental oxygen.
Source: Investigation Report, ¶3
References
(Source material)
Pilot and Passenger Incapacitation, Beech Super King Air 200 VH-SKC, Wernadinga Station, Qld, 4 September 2000, Department of Transportation and Regional Services, Australian Transport Safety Bureau, Investigation Report, 200003771