The crew were hailed as heroes for getting the airplane on the ground without killing anyone. It would soon become apparent that they took an event that should have been nearly routine, an engine relight, and almost lost the airplane with everyone on board. But how could this be? Once again the NTSB report doesn't say, but reading the report objectively leads to a few conclusions. China Airlines did not require unusual attitude recognition and recovery training for its crews, nor did it emphasize cockpit duties delegation during an abnormal situation. The captain had crossed eighteen time zones during six flights in six days and the mishap occurred during his circadian low.
— James Albright
Updated:
2015-03-18

Empennage,
NTSB Report, Figure 8
In the end, the crew flew a textbook approach with a damaged airplane. As one of the passengers said, "The pilot got us into it, but he got us out of it." Yes, I can agree with that. But I have a hard time believing that two fully qualified, experienced pilots could fail to correct an engine loss of thrust with rudder, could fail to recognize the adverse yaw overwhelming the autopilot, could fail to realize three independent attitude indicators were telling the truth, and could fail to recover from an unusual attitude until VMC. Why did they fail so completely? The NTSB report mentions the captain's circadian rhythms and the possibility of desynchronosis — jet lag — as a cause, but did not list it as causal. I'm not so sure.
1
Accident report
- Date: 19 FEB 1985
- Time:
- Type: Boeing 747SP-09
- Operator: China Airlines
- Registration: N4522V
- Fatalities:0 of 23 crew, 0 of 251 passengers
- Aircraft Fate: Repaired
- Phase: En route
- Airports: (Departure) Taipei-Chiang Kai Shek International Airport (TPE/RCTP), Taiwan; (Destination) Los Angeles International Airport, CA (LAX/KLAX), United States of America
2
Narrative
Events
The flight was uneventful until just west of reporting point Redoo, about 300 nmi northwest of San Francisco, California. Flight 006 was at flight level (FL) 410 and was estimating Redoo at 1013. The flight was above a lower cloud layer whose tops were reported to be at or about 37,000 feet. The airplane's autopilot was engaged and was operating in the Performance Management System (PMS) mode. The PMS was providing pitch guidance and maintaining a selected 41,000 feet; roll guidance to the autopilot was provided by the Inertial Navigation System (INS). The autopilot uses only the airplane's ailerons and spoilers for lateral control; it does not use the airplane's rudder and rudder trim for this purpose. The PMS also was maintaining 0.85 Mach (M), 254 knots indicated airspeed (KIAS), by providing thrust setting commands to the airplane's autothrottle system servomotor. According to the flightcrew, as the airplane approached Redoo, it began to encounter light clear air turbulence. The airspeed began fluctuating between about 0.84 (251 KIAS) and 0.88M (264 KIAS) and the PMS began moving the throttles forward and aft to maintain the commanded cruise Mach number (0.85M).
About 1010, the Mach number increased to about 0.88 M, the PMS retarded the throttles, engine thrust decreased to about 1.0 EPR, and the airplane began decelerating. As the airspeed reached about 0.84M, the PMS moved the throttles forward. Engines 1, 2, and 3 responded to the movement of the throttles and began accelerating; however, the flight engineer said that the instrument gauges of the No. 4 engine did not indicate a corresponding acceleration. The flight engineer then moved the No. 4 throttle forward and aft manually, but he said that he did not see any corresponding indication of engine response to the throttle movements on the applicable engine instruments. At the time this occurred, the flight engineer said that the four main tanks were supplying fuel directly to their respective engines. The No. 2 main tank was pressurizing the fuel crossfeed system; all other fuel tank crossfeed valves were closed. The automatic fuel heating system was on. In addition, the captain had turned the "fasten seatbelt" signs on when the flight had encountered the clear air turbulence. In accordance with company procedures, the flight engineer had placed the ignition switches in the "flight start" position, thereby providing continuous ignition to all four engines. At the time of the occurrence, and in accordance with the company's procedures, two of the airplane's three air conditioning packs were on and set to the "half flow" position.
Shortly thereafter, the flight engineer told the captain that the No. 4 engine had flamed out. The flight engineer said that he also noted that the No. 4 generator breaker open light on the electrical section of the flight engineer's instrument panel was lit, indicating that the No. 4 generator control breaker had opened and the generator was no longer on-line. Thereafter, in response to the captain's command, he took out his checklist to review the applicable engine out procedures and the airplane performance charts to ascertain the three-engine enroute cruise altitude. The captain directed the first officer to request a lower altitude from air traffic control (ATC) in order to descend and to restart the engine. Although the maximum engine restart altitude is 30,000 feet, the captain directed the flight engineer to try to relight the No. 4 engine while at 41,000 feet. The flight engineer placed the engine's No. 2 ignition switch to the "flight start" position, thus putting both ignition systems on the No. 4 engine in continuous ignition.
The first officer heard the flight engineer tell the captain that the No. 4 engine had flamed out and he told the relief flight engineer to come forward and help the "on duty" flight engineer. He saw that the airspeed was decreasing and he informed the captain of the situation. At 1014:11, he requested a lower altitude from the Oakland, California, Air Route Traffic Control Center (ARTCC). He did not tell Oakland ARTCC about the engine failure, nor did he declare an emergency. The first officer said that Oakland ARTCC told him to "stand by and he did not recall hearing anything further in response to his request. However, the ATC transcript showed that, at 1015:01, Oakland ARTCC had cleared the flight to descend to and to maintain EL 240 and that Flight 006 did not acknowledge the clearance.
The captain said that the airspeed dropped through 240 KIAS, and, as the airplane continued to decelerate, he turned the autopilot's speed mode selector switch from PMS to "OFF to release it from the altitude hold command. This switched the autopilot to the pitch attitude hold mode while maintaining the INS track in the autopilot roll mode without any pilot input. He then rotated the pitch control wheel on the autopilot manual control module in the nose-down direction to begin a descent to arrest the airspeed loss; however, the captain said that the airspeed continued to decrease and so he disengaged the autopilot to lower the airplane's nose manually at a faster rate in a further attempt to arrest the airspeed loss.
The first officer stated that he "looked up" after he completed his radio call and saw that the airplane had banked "slightly" to the right. He said that he saw the captain disconnect the autopilot, that the airplane continued to bank to the right, and that he "told the captain it was banking right."
The captain said that after he disengaged the autopilot the airplane yawed and rolled further right and that the first officer told him that the airplane "was banking right." He said that while he was concentrating on his attitude director indicator (ADI) to make a left-wing-down correction, the instrument's background, which contained the horizon reference line, rotated rapidly to the left and the horizon reference line rolled to the vertical position. The captain said that he did not see any failure flags or lights on his AD1 and when he looked over at the first officer's AD1 and the standby AD1, they looked the same as his. By this time, according to the captain, the airplane had entered the clouds, and he didn't know what attitude it was in.
The captain said that about the time the ADIs rotated, the flight engineer told him that the other three engines had lost thrust and that the "airplane dropped all of a sudden." He pulled back on the control column, but the indicated airspeed continued increasing rapidly until it exceeded the airplane's maximum operating speed (Vmo). During this part of the "upset," the first officer said that his AD1 had rotated to the left in the same manner as the captain's and that he did not see any AD1 failure flags or lights. He said that, at that point in the flight, he saw that both the captain's and his ADIs "had malfunctioned," that the airplane was out of control, banking left and right, and that he felt that it was in a steep bank.
The flight engineer said that he felt the airplane enter an abnormal attitude, he heard the captain report that his AD1 was lost, and he saw the standby AD1 "going out of limits." He said that the airplane was descending and the captain was trying to recover when he saw the No. 1, 2, and 3 engines had lost thrust. After telling the captain, he moved the three throttles forward and aft, but he did not observe any corresponding indications of thrust response on the engine's instruments. He placed the standby ignition switch "on but there was no engine response. Thereafter, the G forces became so great that he could not lift his arms and his head was forced down against the center control pedestal.
The captain stated that he was unable to recover the airplane while it was in the clouds; he was uncertain of its roll attitude and was moving the control wheel to the left and to the right. However, as the airplane accelerated, the captain said he continued to pull the control column back and the airplane began to decelerate rapidly. The captain said that the airspeed decreased to between about 80 to 100 KIAS and, at that point, he lowered the airplane's nose, the airplane accelerated, and the indicated airspeed again exceeded Vmo. The captain, then assisted by the first officer, pulled the control column back and the airplane decelerated. The captain lowered the nose smoothly. The airplane began accelerating slowly and as it did so, it emerged from the clouds. The captain told the flightcrew that he could see the horizon outside the airplane. The captain, first officer, and flight engineer said that they did not hear the overspeed aural warning and that the stall warning stickshaker did not activate at any time during the descent.
As the airplane emerged from the clouds at about 11,000 feet it was, according to the captain, accelerating through 180 KIAS. The captain, based on outside visual references, began regaining control and was able to finally stabilize the airplane at about 9,500 feet. The first officer said that he saw his AD1 was "coming back" just before the captain announced that he could see the horizon outside the airplane. The flight engineer also noted that he saw the first officer's AD1 "coming in" at this time.
As the airplane descended through 10,000 feet, the flight engineer said that the Nos. 1, 2, and 3 engines "came in," but the No. 4 engine did not start. When he placed the No. 4 ignition switch in the ground start position, however, the engine did start. According to the flight engineer, the restart of the No. 4 engine was accomplished in accordance with checklist procedures.
After the airplane was stabilized, Oakland ARTCC was contacted, and, at 1017:03, Flight 006 reported that it had experienced a "flameout, ah, we . . . emergency. . . .we are niner thousand feet. . ." Thereafter, the flight requested and was given radar vectors to return to course.
After landing, the captain cleared the active runway. Because of the inoperative No. 1 hydraulic system which decreased his ability to steer the airplane during taxi, the captain stopped the airplane after it was clear of the active runway, the engines were shut down, and the airplane was towed to the gate.
Source: NTSB Report, AAR-86/03, ¶1.1
Computer animation
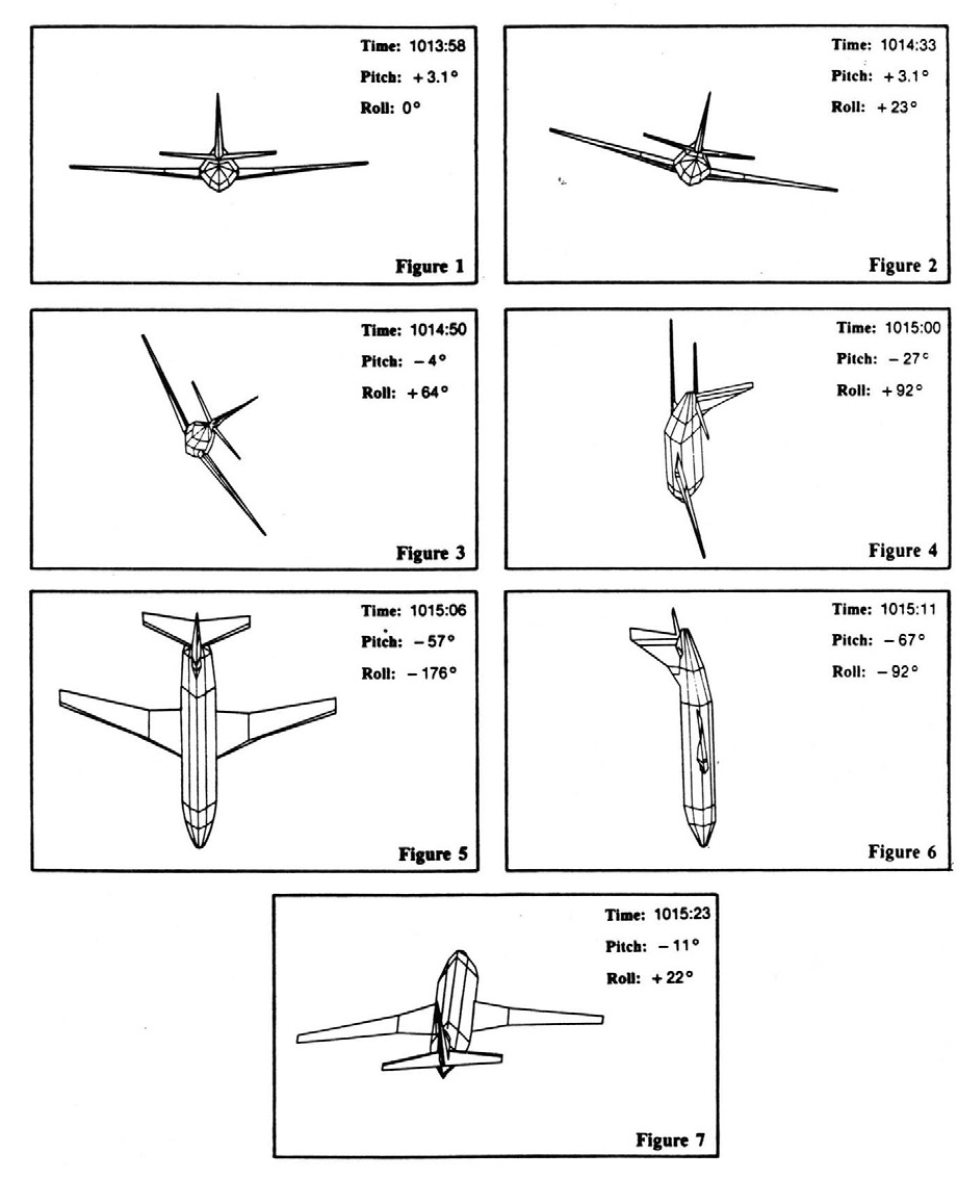
real-time animation of a line drawing of an airplane, driven by selected flight recorder parameters, was prepared.
The presentation depicts the loss of thrust from the No. 4 engine at 40,900 feet. It also shows the increasing left-wing-down control wheel offset to counteract the increasing asymmetric force resulting from the loss of thrust, until the maximum control wheel offset available to the autopilot is reached. The presentation shows that the airplane pitched down and rolled to the right. The nosedown pitch angle reached 69' and, by the time the airplane had descended to 30,000 feet, it had almost completed a 360°right roll and had pitched upward to about ll° nosedown pitch attitude. (Figures 1-7 were extracted from the computer animation.)
Source: NTSB Report, AAR-86/03, ¶1.11
AAR-86/03, figures 1 - 7
Number 4 engine
On February 27, 1985, the No. 4 engine was removed from the airplane and installed in United Air Line's San Francisco main entrance facility's high bypass ratio turbofan engine test cell and subjected to a calibration check to obtain detailed controlled engine performance and transient operating data. The test cell data were evaluated using the manufacturer's computer generated Module Analysis Program, comparing the obtained test data to baseline data obtained from average JT9D-7A production engines.
During engine accelerations above idle, the main fuel control scheduled a fuel flow that was about 200 pounds per hour (pph) toward the lean direction or about 200 pph below expected levels. The engine deceleration time was 0.25 seconds below the minimum acceptable 1.5 seconds and the ground idle speed was about 0.4 percent below the engine's nominal idle trim. In addition, the temperatures supplied to the main fuel control's fuel flow schedule were about 35OF higher than the nominal input values.
[ . . . ] a computer simulation of the engine performance capabilities was conducted using the data obtained during the engine testing and the estimated operating conditions of the airplane at the time of the accident. The simulation showed that if the total estimated air conditioning system bleed air load, coupled with the main fuel control's schedule deviations, were imposed on the engine, the engine would fail to would result in a condition described as "bleed load hogging." During normal engine operation, each engine will supply a proportionate amount of bleed air to the airplane's air conditioning system. If an individual engine remains at or near idle thrust and the remaining engines are operating at higher thrust levels, the engine at or near idle will assume a disproportionate amount of the bleed air load. This bleed load hogging condition raises the engine's "required to run line" and decreases the acceleration rate of the engine. The "required to run linen defines the performance level of an engine in terms of the amount of fuel required to produce a given rpm.
Source: NTSB Report, AAR-86/03, ¶1.16
The captain's duty time
The captain had spent 5 days in Jeddah, Saudi Arabia, before returning to Taipei on February 14, 1985; Taipei time is 5 hours ahead of Jeddah time. He was off duty on February 15; on February 16, he flew a 2 hour 30 minute flight to Tokyo, Japan, returning to Taipei (a 3-hour flight) on February 17. According to the captain, during the nights of February 14 through February 17, he went to sleep between 2100 to 2200 Taipei time and awoke about 0700 to 0800. On February 18, he flew a round trip to Nagoya, Japan, and was off duty 15 hours 20 minutes before reporting for duty on February 19. Flight 006 departed Taipei at 1622 local time and had been airborne about 9 hours 46 minutes when the accident occurred (0214 Taipei time). At the time of the accident, the three primary flightcrew members were on duty. They had been on duty during the takeoff, climb, and initial part of the flight. Thereafter, they each went off duty at intervals ranging from 1 1/2 to, 4 hours after takeoff and were replaced by the augmentee flightcrew members, with the captain occupying the first officer's seat during a portion of this period. The captain was off duty 5 hours during the flight and returned to duty about 2 hours before the accident. During his rest period, the captain slept about 2 hours in the bunk located in the rear of the cockpit.
Source: NTSB Report, AAR-86/03, ¶1.16
3
Analysis
The engine failure
About 1010:46, the PMS, in response to the increased airspeed caused by the wind shear, had decreased the EPRs on all four engines to 0.9 EPR. Then, about 1011:10, the PMS, in response to the now reduced airspeed, began to advance the four throttles to restore the airplane to the commanded 0.85M. The investigation of the No. 4 engine and its components showed that it had experienced a lean shift of the acceleration schedule resulting in a reduction in the fuel flow available for engine acceleration. A reduction of this type reduces the rate a t which the engine would accelerate from flight idle. The DFDR data showed that all four engines started to accelerate; however, the data also showed that the No. 4 engine accelerated at a slower rate than the others. As engines Nos. 1, 2, and 3 accelerated, their respective bleed air controllers closed their 15th stage or high stage bleed air valves. Since the No. 4 engine accelerated slower than the other engines, it did not achieve high enough power for its bleed air controller to close the high stage bleed valve at the same time the high stage bleed air valves were closed on the other engines, and the No. 4 engine, at high altitude, probably assumed most of the air conditioning air bleed load. The additional fuel demand imposed by the "bleed load hogging," in combination with the reduced fuel flow available because of the control lean shift, caused the No. 4 engine to fail to accelerate and to "hang" at slightly above 1.0 EPR.
At some indeterminate time thereafter, the flight engineer decided that the No. 4 engine had flamed out and informed the captain. Between 1012:42 and 1013:04, the No. 4 engine EPR dropped from 1.0 to about 0.7 EPR. By about 1013:09, the No. 4 engine EPR had returned to about 1.0. Based on these data, and the fact that the flight engineer said that he had not moved the engine start lever to cutoff, the Safety Board concludes that engine No. 4 did flame out about 1012:42 and began to decelerate toward windmilling rpm; the subsequent increase in the EPR was caused by inlet spillage from the windmilling engine over the PT2 pressure probe on the strut. The restart attempt was unsuccessful because the attempt was made well above the altitude limits of the inflight airstart envelope.
The Safety Board believes that the Nos. 1, 2, and 3 engines had not flamed out and that the low engine parameters observed by the flight engineer resulted from the throttles being at or near idle.
While there can be little doubt that the loss of thrust on the No. 4 engine was the precipitating factor of the accident sequence, the loss of one engine, albeit an outboard engine, during high altitude cruise should not cause an experienced flightcrew to lose control of their airplane. Indeed, the Airline Operating Manual does not even classify this mishap as an emergency procedure. Therefore, the Safety Board directed its attention to the reasons why the flightcrew was unable to maintain control of the airplane after the loss of thrust on the No. 4 engine.
Source: NTSB Report, AAR-86/03, ¶2.1
The captain's and flight engineer's performances
With regard to the captain and flight engineer, both men were performing in a time spectrum that was later than their typical sleep periods. Although both men had taken a 5-hour rest during the flight, the quality of their rest during this period cannot be equated to that which would have been achieved by sleep either at home or in a hotel. Their duty tasks consisted of routine monitoring of the performance of the airplane's automated flight systems, a task that is repetitive and monotonous and capable of producing a state of boredom.
The flight engineer's performance before, during, and after the loss of control disclosed actions that were correct and timely and other actions that deviated from the required checklist procedure or that demonstrated that he had been unable to analyze correctly the portrayal of the airplane's engine instruments. During the 1 minute 20 second period between the inception of the "hung" engine and the flameout, the flight engineer informed the captain of the status of the engine, moved the throttle aft, then moved it forward to align with the other throttles and awaited the results of the procedure. Since the procedure requires the throttle to be moved slowly and also incorporates a time to interval to wait and evaluate the engine response, the I minute and 20 seconds required to accomplish the task, evaluate the engine response with the captain, and then decide that the engine had either flamed out or had flamed out during his efforts to restore the engine to normal performance were correct and appear to be timely. The facts showed that the flight engineer did not review the alternate operations procedure for this malfunction before trying to restore the engine; however, the AOM states that this procedure may be performed "by recall or references," and also that the AOM may be reviewed before accomplishing the procedure. As a result, the flight engineer did not recall that he was required to close the bleed air valve before manipulating the throttle.
During the descent, the flight engineer had concluded erroneously that the other three engines had flamed out. Several factors led to this misdiagnosis. Shortly after the upset, engines Nos. 1, 2, and 3 were reduced to flight idle thrust. The flight engineer did not move these throttles; thus, when he saw the engine instruments during the dive, the EPRs on engines Nos. 1, 2, and 3 had decreased from their cruise thrust of about 1.5 EPR to flight idle and were nearly aligned with that of the No. 4 engine, which he knew had flamed out.
The Safety Board concluded that a preponderance of the evidence showed that the deviations and omissions noted above resulted from either a lack of knowledge of the airplane systems and procedures, the traumatic effects of the upset and subsequent descent on the flight engineer's ability to scan his instrument panels, or a combination of these two factors.
Since the captain was at the controls when the flight engineer told him that the No. 4 engine did not accelerate, there was no need for him to take any further action other than to monitor the flight engineer's attempts to analyze the engine's performance and restore it to normal operation. He did not disengage the autopilot since it relegated the tasks involved with flying the airplane to merely monitoring the autopilot's performance. Had he disengaged the autopilot, as recommended in his training, he would have been required to perform the physical, more difficult, and more time and attention consuming tasks involved with flying the airplane manually.
The effects of the asymmetrical thrust condition began to assert themselves at about 1011:10, and the No. 4 engine flamed out about 1012:42. Based on the decrease in pitch attitude and the subsequent momentary airspeed increase, the Safety Board concludes that the the PMS was disengaged about 1014:30. Based on the initial movements of the control wheel from its 22.9' left-wing-down position, the Safety Board also concludes that the autopilot was not disengaged until 1014:50. During the 3 minute 40 second period of deceleration, the statements of the captain and flight engineer showed that the captain was totally cognizant of the engine situation, and thereafter, his attention appeared to focus almost exclusively on the airplane's decreasing airspeed. According to the captain, he had disengaged the autopilot in order to lower the nose of the airplane faster and recover airspeed. Although he said that he was aware that the airplane had entered a right bank, he was apparently not aware of the magnitude of the right-wing-down attitude.
The Safety Board concludes that one of the causal factors of the accident was the captain's reliance on the autopilot while the airplane was decelerating. During this 3 minute 40 second period, the captain allowed himself to remain removed from the "control loop by leaving the autopilot engaged. As a result, he was not aware of the increasing control inputs required to maintain level flight. Had the captain placed himself in a "hands on relationship with the airplane by disconnecting the autopilot at the onset of the engine problem, he probably would have been more alert to the increasing asymmetrical forces being exerted on the airplane since he would have been required to make the necessary control inputs to maintain level flight. Since he had no physical relationship with the airplane flight controls, the only cues available to him to monitor the airplane's attitude and performance were the visual cues available from either the airplane instruments or the outside horizon since the airplane was flying above the clouds. However, even under conditions of visual flight, the flight instruments remain the primary tools at high altitudes for maintaining level, stabilized flight in large airplanes. The captain's statement corroborated the fact that he was relying on these instruments for that purpose. Under these conditions, therefore, the primary instrument for attitude control was the attitude director indicator, which may not have concerned the captain initially since it depicted either a wings-level attitude or a very slight left-wing-down bank. With regard to heading, over the period between 1011:09 to about 1014:00, the heading increased about 4¡ a change so slight as to be almost imperceptible. Thus, except for airspeed, which concerned the captain greatly, the only thing in the cockpit that would have depicted the worsening control situation was the control wheel's increasing left wing-down deflection. However, this was an area which was not included in the captain's regular instrument scan pattern, and since he was not "hands on," he was not aware of the deflection.
As noted earlier, an excursion from a stabilized condition might be exaggerated during the transfer from system monitor mode to system controller because time is needed to ascertain the status of the airplane and assess the situation before the pilot can reenter the control loop and take corrective action. When the autopilot was disengaged, the airplane's excursion from the stabilized condition was well advanced and at the point where immediate and proper corrective action was required if the situation was to be remedied safely. The captain was not only unable to assess the situation properly, he was confused by it; therefore, he was unable to take the necessary action to correct the situation. The DFDR data indicated that his actions most probably aggravated the situation. The Safety Board concludes that the captain became spatially disoriented at the onset of the upset and was unable to reorient himself until the airplane began to emerge from the clouds. The fact that the first officer was unable to help the captain reorient himself during the descent showed that he also became disoriented during the upset and descent.
However, the captain was an experienced multiengine and Boeing 747 pilot and he also should have known how the loss of thrust from an outboard engine would affect an airplane's controllability, especially when it is coupled with decreasing airspeed. Given his Boeing 747 experience, the captain should have also known that the autopilot's lateral control authority did not include the rudder and that the effects of the thrust loss could only be counteracted by introducing a left wing-down roll, an action which would also introduce a side slip, increase drag, and aggravate the airspeed decrease.
In conclusion, the Safety Board believes that the loss of thrust on the No. 4 engine was the precipitating factor in the accident; however, we do not believe that it should be considered a contributory factor. Except on takeoff, at, or shortly after critical engine failure speed, an engine loss does not require an emergency procedure wherein immediate and memory actions are required of the flightcrew. An engine loss at cruise altitude and at cruise speeds does not place the airplane in immediate jeopardy nor, for the most part, are any immediate responses required of the flightcrew to retrieve the airplane from jeopardy. The facts of this accident confirm this evaluation since the loss of control did not occur until more than 3 minutes after the No. 4 engine had lost thrust. More than enough time was available to the flightcrew to react properly and prevent the upset. This fact was amply demonstrated on two previous flights for this airplane in which similar situations occurred; the malfunctions were corrected, and the airplane proceeded to scheduled destinations without further incident.
Source: NTSB Report, AAR-86/03, ¶2.2
4
Cause
The National Transportation Safety Board determines that the probable cause of this accident was the captain's preoccupation with an inflight malfunction and his failure to monitor properly the airplane's flight instruments which resulted in his losing control of the airplane.
Contributing to the accident was the captain's over-reliance on the autopilot after the loss of thrust on the No. 4 engine.
Source: NTSB Report, AAR-86/03, ¶3.2
References
(Source material)
NTSB Aircraft Accident Report, AAR-86/03, China Airlines Boeing 747-SP, N4522V, 300 Nautical Miles Northwest of San Francisco, California, February 19, 1985