July 1970, Flying Tiger Line Flight 45, . . . the controller called "At minimum altitude…” The DC-8 continued to descend and broke out of heavy rain and low clouds at an estimated altitude of 75 to 100 feet. The aircraft struck the water . . .
— James Albright
Updated:
2020-07-27

Flying Tiger Line N784FT,
January 7, 1978, Photo: George Canciani
May 1978, National Airlines Flight 193, . . . the aircraft rolled out on the final approach heading, the captain called for the landing gear and the landing final checklist…the ground proximity warning system (GPWS) whooper warning continued for nine seconds until the first officer silenced the warning. Nine seconds later the 727 hit the water . . .
February 1998, Gulfstream III VP-BLN, . . .with 4 nm to go, the crew were cleared to land. The airplane then descended below the glideslope and flew into the water 0.6 nm short of the threshold . . .
June 2006, Learjet 35A N182K, . . . the first officer reported "ground contact," then noted "decision height." The captain immediately reported "I got the lights" which the first officer confirmed. The captain reduced the power to flight idle. Approximately 4 seconds later, the captain attempted to increase power. However, the engines did not have time to respond before the airplane descended into the water . . .
April 2013, Lion Air Flight 904, . . . at 150 ft AGL the captain took over control. The copilot handed the control to the captain and stated that he could not see the runway…the EGPWS called out "Twenty", and the captain commanded a go around. One second later the aircraft impacted the water . . .
September 2018, Air Niugini Flight 73, . . . after passing the Minimum Descent Altitude (MDA), between 307 ft (364 ft RA) fourteen 'Sink Rate' and 'Glideslope' aural alerts began to sound. The flight crew disregarded the alerts, and did not acknowledge the "minimums" and 100 ft alerts. After descending through 100 feet the copilot noticed they were dangerously low and called rapidly with high intonation: "Too low! We’re too low! We’re too low! We’re too low!" The aircraft then skipped across the water several times before it settled in the water . . .
What’s going on here? Why were perfectly good airplanes flown into water short of runways while on approach? And more importantly, why has it continued? July 27th, 2020 is the 50th anniversary since the Flying Tiger Flight 45 crash. The mistakes they made fifty years ago are still being made today. Clearly the lessons haven’t been taken to heart. So, let’s do that. Let’s case study Flying Tigers Flight 45, and take to heart the lessons contained:
1
Accident report
- Date: 27 July 1970
- Time: 11:36
- Type: McDonnell Douglas DC-8-63AF
- Operator: Flying Tiger Line
- Registration: N785FT
- Fatalities: 4 of 4 crew, 0 of 0 passengers
- Aircraft Fate: Destroyed
- Phase: Approach
- Airport: (Departure) Tokyo-Haneda Airport (HND/RJTT), Japan
- Airport: (Destination) Okinawa-Naha AFB (AHA), Japan
2
Narrative
Narrative
The flightcrew involved in the accident arrived in Tokyo on Flight 43 at 2032, July 26, 1970, after a flight of 6.2 hours from Cold Bay, Alaska. They checked into their hotel in Tokyo at 2124 and were called at 0630 the next morning to prepare for departure on Flight 45. The scheduled departure time for Flight 45 was 0740 but due to crew rest requirements the departure time was rescheduled for 0900. The crew boarded the aircraft about 0830, and after additional delay took off at 0929 for Naha Air Base, Okinawa.
Two hours after takeoff, following an en route descent to 1,000 feet m.s.l., Naha Control established radar contact with the aircraft. At the time radar contact was established (1129) the flight was 18 miles northwest of the airport aid was apparently operating in visual meteorological conditions, as they had been during virtually the entire flight from Tokyo. At 1131 the controller advised: "…have reduced visibility on final…tower just advised approach lights and strobe lights are on…" Cockpit conversations reflected the crew's displeasure with the location of reduced visibility due to shower activity.
Meteorological Information
The weather at the Naha Air Base, 8 minutes prior to the accident, was reported to be: ceiling 1,500 feet, visibility 7 miles in light rain showers, winds variable at 5 knots, towering cumulus overhead and in all quadrants, altimeter setting 29.84 inches, visibility to the north 1 mile. Scattered stratus clouds were reported at 1,000 feet and broken cumulus clouds at 1,500 feet. A weather observation taken about 4 minutes after the accident was: ceiling 1,500 feet, visibility 10 miles in light rain showers, wind 360° at 8 knots, altimeter 29.83 inches, visibility to the north 1.5 miles. Scattered cumulonimbus and broken cumulus clouds were reported at 1,500 feet. Cumulonimbus were reported northwest-northeast of the station and stationary towering cumulus were existent in all quadrants.
A U.S. Air Force C-130 completed a ground-controlled approach (GCA) to Runway 18 at Naha several minutes before Flight 45 commenced its approach. The C-130 pilot subsequently reported that during his approach there was a heavy rain shower, approximately 1 mile in diameter, extending 1/8 to 1/4 of a mile west of the extended centerline of Runway 18, and immediately north of the approach end of the runway in the vicinity of the GCA minimum altitude position. He estimated that visibility was less than a mile in the rain shower but said that no turbulence was encountered in the shower.
Ground witnesses also reported that at the time of the crash, a heavy rain shower existed immediately north of the approach end of Runway 18. One described the shower as having a "wall-of-water" appearance in contrast to the surrounding light or nonprecipitation areas.
The light conditions at Naha at the time of the accident were those associated with a broken cumulus cloud cover, clear areas of bright noonday sunshine, and a dark area north of the field where the rain shower was located.
Aids to Navigation
The only available means of conducting an instrument approach to Runway 18 at Naha was the use of precision approach radar.
Source: Paraphrased excerpts from NTSB-AAR-72-10
For more on Precision Approach Radar: PAR.
Naha precision approach radar (PAR) minima as specified in the instrument approach chart for the Flying Tiger Line, Inc., were 300 feet and 3/4 mile visibility for all turbo jet aircraft. U.S. Air Force PAR minima were 200 feet and 1/2-mile visibility, and published as such in Department of Defense flight planning publications.
Narrative (continued)
At slightly less than 5 miles from touchdown, the crew was instructed to begin the descent onto glidepath and was cleared to land. The approach continued, with various heading changes and, at 1134:53, the crew was advised that they were slightly below the glidepath, 3 miles from touchdown. Additional vectors were provided and, at 1135:07; a sound, similar to the blowing of rain removal air, began; this sound continued at a steady level to the end of the CVR recording.
At 1135:14, 2 miles from touchdown, the crew was advised "…dropping slightly below glidepath…you have a 10 knot tailwind." At 1135:34, the controller advised the crew that they were on glidepath.
At 1135:37, the controller advised the flight, "One mile from touchdown, slightly left of course, turn left heading one eight five - turn left heading one eight two."
The crew adhered closely to heading and altitude instructions until level off upon reaching Flying Tiger minimums (300 feet). Thereafter, however, the aircraft descended through the Decision Height.
At 1135:42, an unidentified person in the cockpit said, "hundred feet." At 1135:43, the controller said "At minimum altitude, going well below glidepath, too low…” At 1135:44, during the above transmission an unidentified person in the cockpit said, "seventy feet" and, at 1135:44.5, he said, "It's fifty feet." The last comment was ended at 1135:45.5 by an electrical interruption to the recorder, and all recording stopped at 1135:46.
Ground witnesses reported that the aircraft broke out of heavy rain and low clouds at an estimated altitude of 75 to 100 feet.
The aircraft struck the water approximately 2,200 feet short of the runway threshold lights. The water in the accident area varied in depth from 6 to 70 feet.
A witness, who was fishing near the point where the aircraft struck the water, was one of the first to arrive at the cockpit section. He stated that upon his arrival there were two survivors whom he later identified by photographs as the first and second officers. These two officers subsequently died from drowning, the navigator died from asphyxiation, and the captain from traumatic head injuries.
Persons who arrived on the scene several minutes after the accident spoke with the first officer. He had access to a small hole torn in the underside of the fuselage and could talk to the would-be rescuers. One witness stated, that in response to queries as to what had caused the accident, the first officer said, "Everything was okay until we hit."
Source: Paraphrased excerpts from NTSB-AAR-72-10
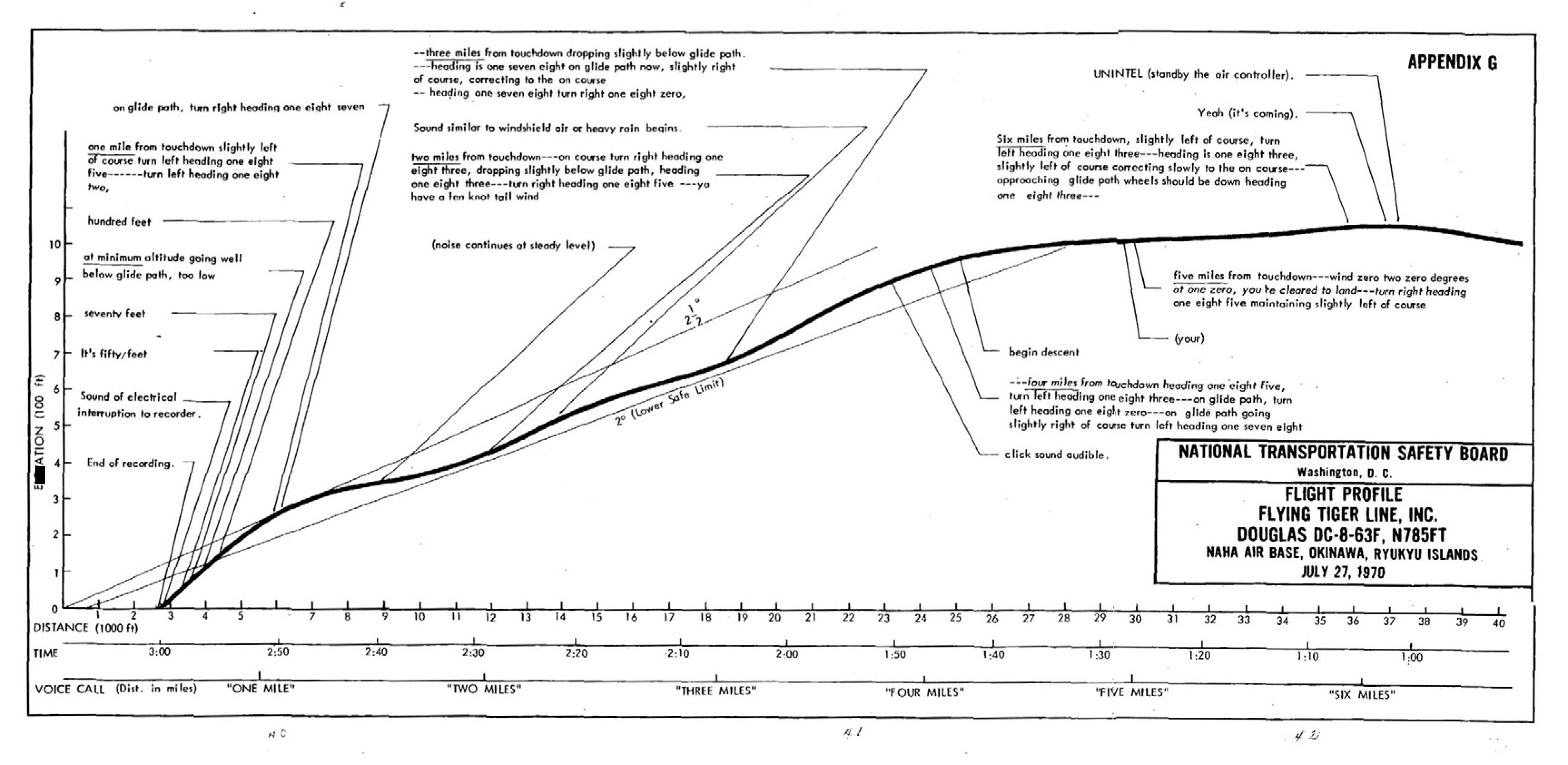
Flight Profile, NTSB AAR 72-10, Appendix G
The initial rate of descent onto the glidepath stabilized at about 950 feet per minute (f.p.m.). At slightly more than 3 miles, the rate of descent decreased to about 750 f.p.m. At the point where the CVR began recording a sound similar to the blowing of rain removal air the rate of descent increased to about 940 f.p.m. and continued at that rate until the level-off maneuver began about 8 seconds later. Following the 7-second period of nearly level flight, the aircraft began to descend at an ever increasing rate during the final 17 seconds of flight; the rate of descent averaged about 1150. f.p.m. during those seconds.
Source: Paraphrased excerpts from NTSB-AAR-72-10
The initial descent was too high to capture the 2-1/2° and the crew maintained a glide path closer to 2° until given a “dropping slightly below glide path” notification. At that point the pilot appeared to level off to intercept the glide path and then descended aggressively, perhaps spotting the approach lights.
3
Analysis
The crewmembers were all performing their duties and conversing in normal tones until just before the accident occurred.
The crew adhered closely to heading and altitude instructions until level off upon reaching Flying Tiger minimums (300 feet). Thereafter, however, the aircraft descended through the Decision Height and contacted the water. Accordingly, the investigation was directed toward determining what factors may have led to this unwarranted descent.
As the aircraft progressed into the rain shower, the crew probably lost external visual reference completely, due to the intensity of the rain. However, since the flight was nearing approach minimums and they expected to break out of the shower momentarily, the captain undoubtedly devoted his attention to locating the approach lights.
During the 7-second period of level flight at 325 feet m.s.l. the aircraft passed through the most intense portion of the shower and emerged into an area of increased light intensity. The backlighted light rain' could well have caused visual disorientation effects associated with an illuminated high intensity "Ganzfield" phenomenon (a homogeneous visual field of similar brightness in which no differentiating objects can be seen). The glare not only would preclude reference to outside objects but also would limit reference to cockpit instruments. During this period the final approach controller advised the crew that they were "on glidepath" and had a 10 knot tailwind. The "on glidepath" transmission undoubtedly reassured the crew regarding their altitude and position.
About 8 seconds after this "on glidepath" portion of the controller's transmission, an unidentified person in the cockpit (probably the second officer) called out "hundred feet." At that point the flight recorder indicated an altitude of 85 feet m.s.l. There was no evidence that this call alarmed the captain or the first officer, even though the radar altimeters would have indicated the altitude. The amber warning lights associated with these radar altimeters would have been lit also, since the captain's reference "bug" was set at 200 feet m.s.l. and the first officer's was set at 300 feet m.s.l.
One second after the "hundred feet" call the controller advised the flight: "at minimum altitude, going well below glidepath, too low…" The CVR recording of the controller's instructions ended at that point. While the final approach controller was making that transmission, the unidentified person in the cockpit was calling, "Seventy feet" and "It's fifty feet." If the latter calls alarmed the captain and/or the first officer, it was too late to refocus on the instruments, interpret them, and effect a recovery from the relatively high rate of descent that existed during the last few seconds of flight.
During the period from 1134:14 (5 miles from touchdown) to 1135:37 (1 mile from touchdown and 8.5 seconds prior to impact), the controller gave the flight six heading changes. The first officer was required to concentrate on making directional changes which may have precluded an effective overall surveillance of other instruments, particularly the altimeter. Thus, he may have been relying on the controller to provide altitude information. There was no evidence that either the "500 feet above minimums" or "100 feet above minimums" call, required by company directives, was made…Also, there was an evident lack of a clear understanding between the pilots as to what the DH should be. The first officer determined correctly that the DH was 300 feet (314 feet m.s.l.) as his radio altimeter bug was found set at 300 feet; he had leveled the aircraft at about 325 m.s.l. for a period of 7 seconds; and the altitude reminder dial was found set at 310 feet. The captain apparently had a minimum altitude of 200 feet in mind. His radio and pressure altimeter bugs were found set at 200 feet. Assuming that the captain intended to make the "100 feet above minimums" call, a normally accepted procedure, he could not have been expected to make the call since the aircraft did not reach the 100-foot point (314 feet m.s.l.) above his 200 feet minimums until the aircraft departed the level-off altitude of 325 feet. During the reinitiated descent, his attention probably was devoted to locating the runway.
Findings
- Flying Tiger Line, Inc., precision approach radar minimums for Naha Air Base were 300 feet and 3/4-mile visibility.
- The approach was flown to DH in accordance with the final controller's instructions.
- There was a heavy rain shower in the vicinity, approximately 1 mile in diameter, at minimum descent altitude. The area surrounding the rain shower was brightly lighted by midday sunlight.
- The required approach altitude calls were not made.
- The captain's radio altimeter reference bug was set improperly at 200 feet, the first officer's was set correctly at 300 feet, and the altitude reminder dial was set at 310 feet.
- The aircraft leveled at about 325 feet m.s.l., and power was reduced. Power was never increased thereafter.
- Correlation of the CVR and FDR information showed that someone in the cockpit called out "Hundred feet" at the same time the aircraft was at 100 feet m.s.l.
- No action was taken by either pilot when this call was made.
- The aircraft was seen emerging from the rain shower 75 to 100 feet above the water.
- The aircraft contacted the water 2.5 seconds after the beginning of the "at minimums" call by the final approach controller.
- Meteorological conditions created a veiling glare and a visual field of similar brightness.
Source: Paraphrased excerpts from NTSB-AAR-72-10
4
Cause
The National Transportation Safety Board determines that the probable cause of this accident was an unarrested rate of descent due to inattention of the crew to instrument altitude references while the pilot was attempting to establish outside visual contact in meteorological conditions which precluded such contact during that segment of a precision radar approach inbound from the Decision Height.
Source: NTSB-AAR-72-10
5
Additional Thoughts
Veiling Glare Explained
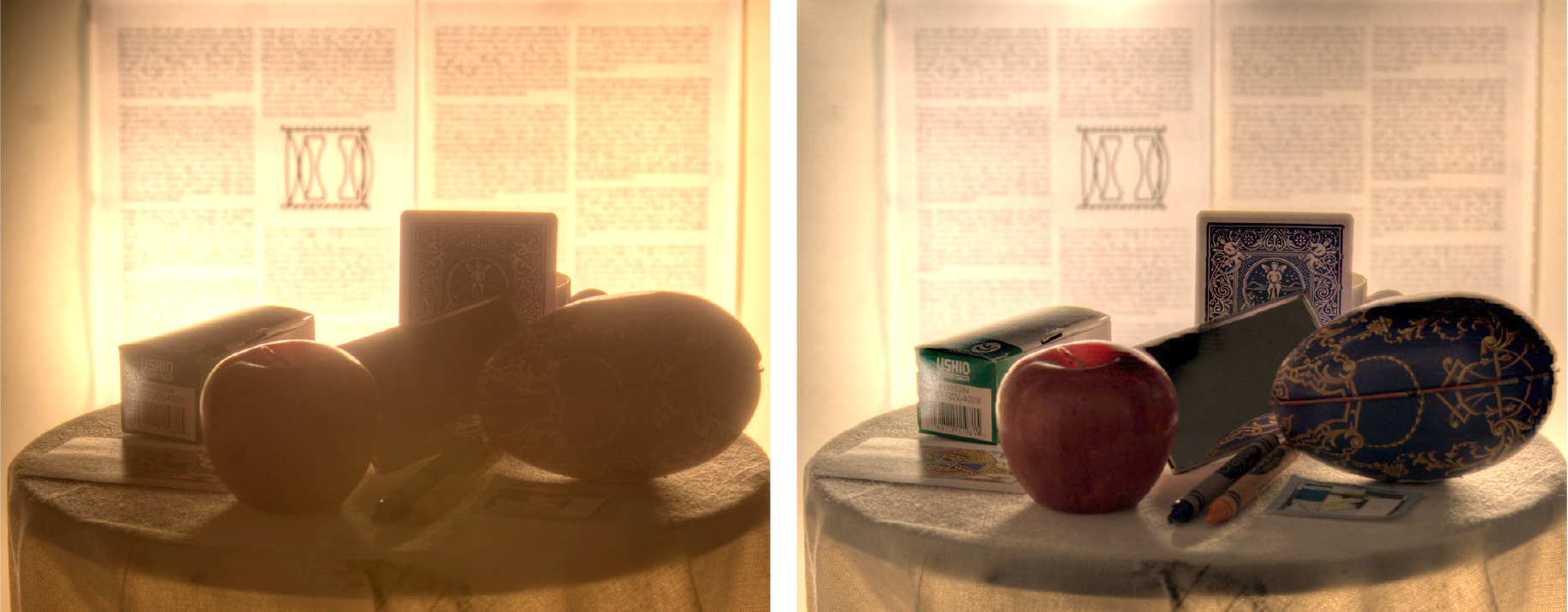
Talvala, Two images of a strongly back-lit scene, veiling glare on the left
Veiling glare is a term normally used in photography to denote a distortion caused by a camera's inability to provide contrast between brightly lit areas and shadows. it is also used as a medical term for glare resulting from excessive illumination.
The Veiling Glare Hypothesis
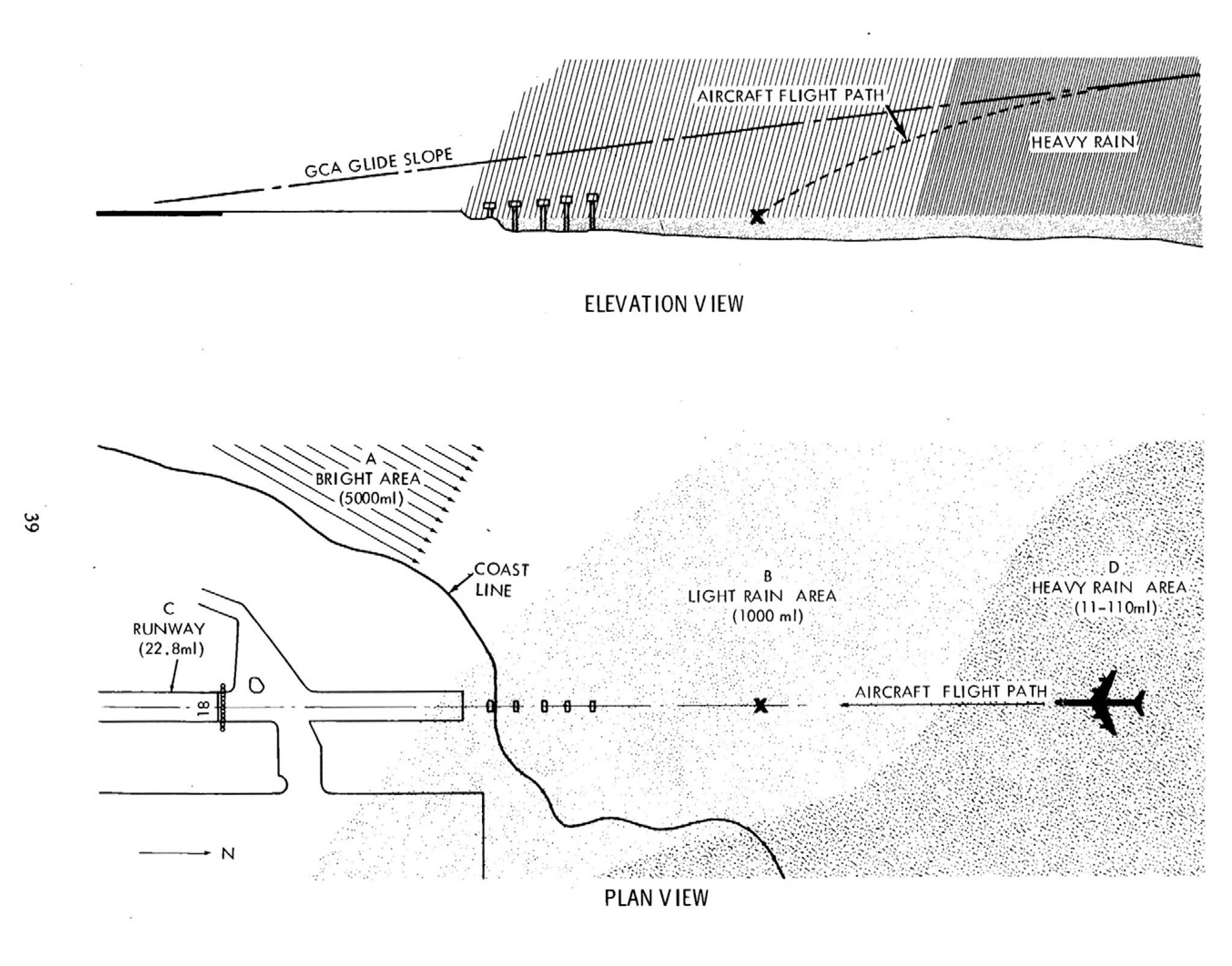
Elevation and plan views, NTSB-AAR-72-10, Appendix F
On emerging from the heavy rain shower the pilots have entered the area of relatively high brightness between them and the runway, after having been in an area of about 11 ml. to 110 ml. brightness for some 30 seconds or more. Some dark adaptation would therefore have begun but in 30 seconds it would have been minimal. However, under the circumstances, exterior visual references on which to fixate or accommodate would have been nonexistent on transference of vision from inside to outside the cockpit. Although men of the pilots' ages, wearing near vision corrective lenses, would have had to accommodate by only one diopter at most, recent data indicates that this would require from 6 to 8 seconds. With the lack of anything outside the cockpit on which to focus the eyes, incomplete focusing would result. This along with the sudden appearance of the relatively high brightness of the back-lighted rain would have effectively presented the pilots with an illuminated Ganzfield.
Unlike total darkness wherein one does not expect to see things, the lighted Ganzfield often makes the individual conscious of both the severe visual disorientation present and the uncertainty as to where he is looking. In this instance, such a condition would have produced a very serious problem for pilots hurriedly attempting to locate a single object - the runway. It has been shown that under similar experimental conditions, observers took as long as 20 seconds to locate an object six times larger than a runway threshold.
Consequently, under the meteorological conditions present at the time of the accident, the pilots may have been faced with a series of phenomena, any one of which, by itself, would not have precluded visual acquisition of the runway. However, when combined together as (1) the veiling glare, (2) restricted optical range, (3) incomplete visual accommodation, and (4) the sudden appearance of a back-lighted, high intensity Ganzfield with its possible disorientation effects, it would appear that acquisition may have been effectively denied.
Source: NTSB-AAR-72-10, Appendix F
Application
What are your thoughts? How could this accident have been prevented? What are the key takeaways from this accident that we can apply to our flying? Four stand out to me:
First, as demonstrated by this accident and numerous others, any approach made over open water presents distinct challenges and hazards due to unique optical illusions and lack of depth perception. No descent below DA/MDA should be made without clearly identifying the runway environment with enough detail to accurately judge a safe descent path angle to the runway.
Second, this accident reemphasizes the safety benefits of a Stabilized Approach for precision approaches and CDFA for non-precision approaches. The pilot’s last-minute correction back to the glide path just before spotting the lights meant he went through a number of pitch and power changes and the last moments depended on the pilot establishing a sight picture of the landing environment and making the necessary adjustments. As the veiling glare hypothesis points out, this is incredibly hard to do. One of the benefits of the stable approach is that once you’ve got the airplane aimed to the touchdown point, the next move should be to reduce power and flare. If you find yourself doing something other than that prior to getting to the flare, you’ve done something wrong and a go around is well advised. This is always important on a low visibility approach, but especially so during a PAR where you have no visual clues about the glide path.
Third, while briefing an approach, include a discussion of the anticipated weather conditions. Identify any specific hazards and develop risk mitigation strategies.
Fourth, strict adherence to standard operating procedures and defined PF/PM roles are essential. This accident clearly demonstrates what can happen when a lapse of adherence to defined roles occurs.
Fifty years ago Flying Tiger Line Flight 45 faced a challenging approach. You can be sure your future will be filled with challenging approaches too. Be ready for it.
References
(Source material)
NTSB Aircraft Accident Brief, AAR-72-10, Flying Tiger Line, Inc. Douglas DC-8-63F N785FT, Naha Air Base, Okinawa, Ryukyu Islands, July 27, 1970
Talvala, Eino-Veille, etal, Veiling Glare in High Dynamic Range Imaging, Standford University, undated