There is a fascinating television program about this incident. "Mayday: Ghost Plane" romanticizes the role of a flight attendant who managed to get into the cockpit and almost saved the day but perhaps lost his will after discovering his girlfriend, another flight attendant on board, had died. It also makes an issue of the captain's belittling of the first officer, shutting him down and possibly rushing him through his preflight duties. None of this is supported in the accident report, but it does make for good T.V.
— James Albright
Updated:
2021-00-00
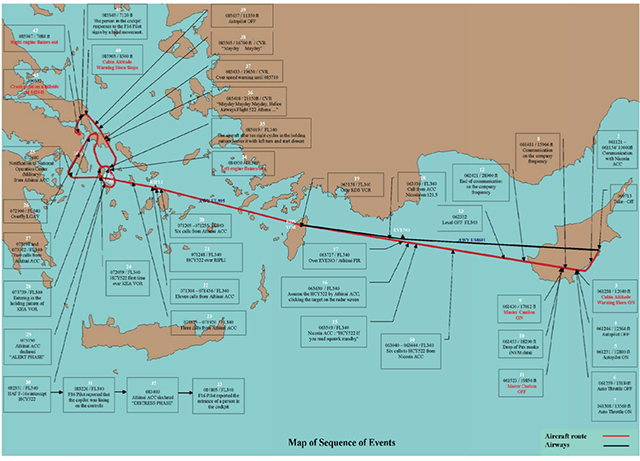
Sequence of Events Map,
from Accident Report, pg. 8.
The report does note CRM issues and does a good job of figuring out what happened. It makes for good reading, but here is the abbreviated version:
- The airplane had a history of pressurization problems.
- The mechanic didn't failed to properly apply the maintenance procedure that would have verified the pressurization leakage and failed to return the pressurization switch from its manual position to the automatic position.
- The first officer, who had a history of SOP problems, failed to detect the improperly set switches.
- The aircraft was designed with a warning horn that had two meanings: on the ground it meant takeoff configuration and in the air it meant high cabin altitude. The captain misinterpreted it and continued to trouble shoot while continuing the climb and failing to don oxygen.
- Everyone eventually passed out, the aircraft ran out of gas, all aboard were killed.
Regardless of which version you believe — the romantic Hollywood tale or the cold facts of the accident report — there are several lessons we can take away from this mishap:
- Fuselage pressure leaks should be addressed immediately and repaired.
- Oxygen supply and delivery equipment must be pre-flighted.
- During every climb, part of your 10,000 foot check must be a check of cabin altitude. Most airplanes have a maximum cabin altitude between 6,000 and 8,000 feet. You certainly should not be above that at 10,000 feet aircraft altitude. You should know your normal cabin climb rate, typically around 300 fpm. Even if it takes you ten minutes to get to 10,000 feet aircraft altitude, you should not see more than 3,000 feet cabin altitude at that point. In any case, if it isn't where it should be, level off and investigate.
- When troubleshooting a pressurization problem, donning oxygen quickly will not only improve your mental capabilities, it can keep you in the game if things go south quickly or insidiously.
- When in doubt, descend.
1
Accident report
- Date: 14 August 2005
- Time: 12:03
- Type: Boeing 737-31S
- Operator: Helios Airways
- Registration: 5B-DBY
- Fatalities: 6 of 6 crew, 115 of 115 passengers
- Aircraft Fate: Destroyed
- Phase: En route
- Airports: (Departure) Larnaca Airport (LCA/LCLK), Cyprus
- Airports: (Destination) Athens-Eleftherios Venizelos International Airport (ATH/LGAT), Greece
2
Narrative

Pressurization Panel, from Helenic Republic Accident Report, pg. 51.
Post crash analysis determined the switch was actually in the "MAN" position from before the flight, during the flight, until impact when it was knocked into the position shown. (Actual switch position was recorded by non-volatile memory.)
- On 13 August 2005, on the flight prior to the accident, the Helios Airways (the Operator) Boeing 737-300 aircraft, Cyprus registration 5B-DBY, departed London-Heathrow, United Kingdom for Larnaca, Cyprus at 21:00 h. The aircraft landed at Larnaca at 01:25 h on 14 August 2005.
- During the flight, the cabin crew noted a problem with the right aft service door. The cabin crew made an entry in the Aircraft Cabin Defect Log that “Aft service door (starboard) seal around door freezes & hard bangs are heard during flt [flight]”. The write-up by the cabin crew was transferred to the Aircraft Technical Log by the flight crew as “Aft service door requires full inspection.”
- Immediately after the arrival of the aircraft in Larnaca, the authorized company Ground Engineer (number one) went to the Boeing 737 aircraft for the required inspections. He performed a visual inspection of the aft service door and he carried out a cabin pressurization leak check. In response to the write-up in the Aircraft Technical Log, the Ground Engineer documented his actions as follows: “Door and local area inspected. NIL defects. Pressure run carried out to max diff. Safety valve operates at 8.25 No leaks or abnormal noises (IAW MM 21 – 32 – 21 – 725 – 001)”.
- The aircraft took off from Larnaca airport at 06:07:13 h. At 06:11:21 h, the flight crew contacted Nicosia Area Control Centre (ACC) at reporting point LOSOS, climbing through flight level (FL) 100 for FL 200. At 06:11:35 h, Nicosia ACC identified the flight and asked for the requested final cruising level. The Captain requested cruising level 340. At 06:11:45 h, flight HCY522 was cleared to climb to FL 340 and to proceed direct to the RDS (Rodos) VOR. The Captain acknowledged the clearance. This was the last recorded communication between the flight crew and Nicosia ACC.
- According to the Flight Data Recorder (FDR), at 06:12:38 h and at an aircraft altitude of 12 040 ft and climbing, the cabin altitude warning horn sounded. At 06:14:11 h, at an aircraft altitude of 15 966 ft, the Captain contacted the company Operations Centre on the company radio frequency, 131.2 MHz. According to the Operator’s Dispatcher, the Captain reported “Take-off configuration warning on” and “Cooling equipment normal and alternate off line.” The Dispatcher requested an on-duty company Ground Engineer to communicate with the Captain.
- During the communication between the flight crew and the company Operations Centre, the passenger oxygen masks deployed in the cabin as they were designed to do when the cabin altitude exceeded 14 000 ft. It was determined that the passenger oxygen masks deployed at 06:14 h at an aircraft altitude of approximately 18 000 ft (extrapolation of the data from the NVM in the cabin pressure controller).
- According to the FDR, the microphone keying (communication between the Captain and the Ground Engineer) ended at 06:20:21 h as flight HCY522 was passing through 28 900 ft. Shortly afterwards, the Operator’s Dispatcher called the flight crew again but there was no response.
- At 06:23:32 h, the aircraft leveled off at FL 340.
- At 07:20:59 h, the flight passed the KEA VOR, and began what appeared to be a standard instrument approach procedure for landing at Athens International Airport, runway 03L, but remained at FL 340. At 07:29 h, flight HCY522 flew over the Athens International Airport still at FL 340 and following the missed approach procedure for runway 03L turned right towards the KEA VOR. At 07:37:39 h, flight HCY522 reached the KEA VOR and entered the published holding pattern.
- At 08:23:51 h, during the sixth holding pattern, flight HCY522 was intercepted by two F- 16 fighter aircraft of the Hellenic Air Force. The F-16s made close visual contact with the flight in the holding pattern, at FL 340. During the interception, the F16s communicated on the military radar frequency and with Athinai ACC. One of the F-16 pilots attempted to attract the attention of the flight crew using prescribed interception signals and radio calls on the emergency and Athinai ACC frequencies, without success. He maneuvered around the aircraft to acquire various views from the right and left sides of the cockpit and the fuselage in an effort to identify the reasons for the lack of radio communication. No external structural damage or fire/smoke was observed.
- At 08:32 h, the F-16 pilot reported by radio that the Captain’s seat was vacant. The First Officer’s seat was occupied by someone who was slumped over the controls. Two passengers on the left side of the aircraft, one wearing white clothing and the other red clothing, sat motionless in their seats and were wearing oxygen masks on their faces. Additional oxygen masks could be seen dangling from their overhead units. The passenger cabin was dark, but the shadow of the oxygen hoses and masks could be seen against the daylight shining through the windows on the other side of the passenger cabin. Another passenger was seen from the right side of the aircraft wearing white clothing, sat motionless and wore an oxygen mask.
- At 08:48:31 h, two chimes were heard on the CVR and, at 08:48:51 h, another two chimes were heard followed after 20 seconds by a continuous chime which lasted 20 seconds. Some seconds later, a click sound similar to the cockpit door opening was recorded. Also, sounds similar to movement in the cockpit, seat adjustment, and oxygen mask removal from its stowage box and oxygen flow during donning of the mask were recorded.
- Approximately 08:49 h, during the tenth holding pattern, the F-16 pilot observed a person wearing a light blue shirt and dark vest, but not wearing an oxygen mask, enter the cockpit and sit down in the Captain’s seat. He put on a set of headphones and appeared to place his hands on the panel directly in front of him.
- According to the FDR, at 08:49:50 h, the left engine flamed out. At this time, the F-16 pilot observed what he assumed was fuel coming out of the left engine. The aircraft turned steeply to the left and headed in a northerly direction. The person in the Captain’s seat did not respond to any of the attempts of the F-16 pilot to attract his attention. He appeared to be bending forward every now and then. Flight HCY522 began a descent on a northwesterly heading. The two F-16s followed at a distance due to the maneuvering by the Boeing 737.
- When the F-16 pilot next came close to the Boeing 737, he saw the upper body of the person in the First Officer’s seat lean backwards as if he was sitting up. It became evident that this person was not wearing an oxygen mask and remained motionless.
- At 08:54:18 h, the following distress was recorded by the CVR “MAYDAY, MAYDAY, MAYDAY, Helios Airways Flight 522 Athens ... (unintelligible word)”. A few seconds later, another “MAYDAY, MAYDAY” with a very weak voice was recorded.
- When the Boeing 737 was at about 7 000 ft, the person in the Captain’s seat for the first time appeared to acknowledge the presence of the F-16s and he made a hand motion. The F-16 pilot responded with a hand signal for the person to follow him on down towards the airport. The person in the Captain’s seat only pointed downwards but did not follow the F-16.
- At 08:59:20 h, the heading of the Boeing 737 changed to a southwesterly direction. The aircraft continued to descend. At 08:59:47 h, according to the FDR, the right engine flamed out at an altitude of 7 084 ft.
- The aircraft continued to descend rapidly and collided with rolling hilly terrain in the vicinity of Grammatiko village, approximately 33 km northwest of the Athens International Airport at 09:03:32 h.
Source: Helenic Republic Accident Report, ¶1.1
3
Analysis
- The Captain was male, 59 years old.
- The Captain had worked for the Operator for two separate time periods. According to interviews of his peers at the Operator, during the first period, he presented a typical “command” attitude and his orders to the First Officers were in command tone. During the second period, his attitude had improved as far as his communication skills were concerned.
Source: Helenic Republic Accident Report, ¶1.5
He had been an airline pilot for various operators for 35 years with nearly 17,000 hours
- The First Officer was male, 51 years old.
- According to statements by his next of kin, colleagues and friends, the First Officer was an optimist, calm, active and a social person. He had expressed his views several times about the Captain’s attitude. He had also complained about the organizational structure of the Operator, flight scheduling and he was seeking another job.
Source: Helenic Republic Accident Report, ¶1.5
He had 19 years of experience, mostly as a second officer, with just over 7,500 hours. He had a reputation for having difficulties with complex tasks, checklist discipline, and standard operating procedures..
- According to Technical Log entries, unscheduled maintenance tasks were performed at Larnaca on 19 December 2004 by an authorized Ground Engineer of ATC Lasham, in order to investigate the cause of a rapid decompression which had occurred on 16 December 2004, as described in paragraph 1.18.1.1. It should be noted that this event occurred just 07:31 flight hours and seven landings after a “C” check performed on 10 December 2004.
- Maintenance action was taken by the authorized Ground Engineer at Larnaca airport in response to the pilot write-up in the Aircraft Technical Log (p. 650): “Rapid decompression. Descent to 10 000. Pax O2 deployed.” As a result of the maintenance action taken, the Ground Engineer recorded the following corrective actions: “Aft R/H service door adjusted and rigged acc to MM adjustments and test procedure 52-41-00.”
Source: Helenic Republic Accident Report, ¶1.6

- The left engine bleed toggle switch (BLEED 1) was found in the OFF position. The right engine bleed toggle switch (BLEED 2) was visually found in the OFF position. The APU toggle switch was found in the OFF Position. The isolation valve toggle switch was found in the AUTO Position. The left air conditioning pack switch appeared to be in the AUTO position. The position of the right pack switch could not be determined because of impact damage.
Source: Helenic Republic Accident Report, ¶1.12.2
- The cabin pressure controller contained a Non-Volatile Memory (NVM) chip that recorded pre-determined data and flight events during flight. The NVM contained data from 42 records, which was the maximum capacity of the NVM.
- The NVM recording showed that on the accident flight, the cabin pressure control system was being operated in the manual mode. The aft OFV was constant at a 14.6 degree opening angle as measured from the fully closed position, and the flight mode was CLIMB. This was also approximately the position of the outflow valve actuator found at the accident site. Cruise flight level was selected to FL 340 and the landing field elevation to 350 ft. The Cargo Heat Valve (also known as Forward Outflow Valve) and both Pack Valves and Bleeds were indicated NOT CLOSED.
- The recorded data for aircraft altitude, cabin altitude, aircraft rate of climb, cabin rate of climb, and outflow valve position on flight leg 8984 (which was the last flight) were as follows:
- At an aircraft altitude of 12 500 ft, the cabin altitude was 10 000 ft. The aircraft rate of climb was 2 939 ft / min and the cabin rate of climb was 2003 ft / min with a constant aft OFV opening angle of 14.6 degrees as counted from the fully closed position. The differential pressure was 0.936 psi and the flow of air through the aft OFV was 41.10 lb/min.
- At an aircraft altitude of 16 650 ft, the cabin altitude was 13 500 ft. The aircraft rate of climb was 2 831 ft / min and the cabin rate of climb was 2304 ft / min with the valve angle 14.64 degrees constant. The differential pressure was 1.05 psi and the flow of air through the aft OFV was 40.50 lb / min.
- At an aircraft altitude of 18 200 ft, the cabin altitude was 14 700 ft. The aircraft rate of climb was 3 306 ft / min and cabin rate of climb was 2 523 ft/min. The outflow valve angle was constant at 14.54 degrees open from the fully closed position. The differential pressure was 1.117 psi and the flow of air through the aft OFV was 39.95 lb / min.
- There was no indication of any cabin pressure control system related malfunction or problem in any of the data recorded on the NVM.
- According to the NVM data, the cabin altitude of flight HCY 522 during the climb was as follows:
- At flight level 12 500 ft, the cabin altitude was 10 000 ft;
- At flight level 16 650 ft, the cabin altitude was 13 500 ft; and
- At flight level 18 200 ft, the cabin altitude was 14 700 ft;
- According to the FDR data, the cabin altitude warning horn sounded 2 – 3 seconds before the NVM data recorded a cabin altitude of 10 000 ft. Similarly, the FDR recorded a MASTER CAUTION at an aircraft altitude of 17 000 ft (the cabin altitude was approximately 13 800 ft). The MASTER CAUTION was probably triggered by either the passenger oxygen masks deployment or illumination of the equipment cooling light.
- Based on calculations by Nord-Micro, the final cabin altitude was estimated by extrapolation to have reached approximately 24 000 ft. Based on similar calculations, the Boeing Company estimated the final cabin altitude to have been between from 20 500 ft to 28 200 ft.
- The cabin pressure mode selector was confirmed to be in the MAN (manual) position by physical witness marks on the mode selector input shaft and by electrical continuity checks in the mode select circuitry.
Note.- The air flow rates through the aft OFV are calculated values derived from the recorded outflow valve position and differential pressure.
Source: Helenic Republic Accident Report, ¶1.16
- The NASA Aviation Safety Reporting System (ASRS) conducted a search of its database for incidents similar to the accident flight. The result of the search yielded 171 reports of air conditioning and pressurization problems that involved Boeing 737 aircraft in the past decade (1994-2004). Of the 171 reports, 58 were deemed critical. According to Boeing, the rate of reports per a million departures was 2.7.
- Of interest and relevance to the accident under investigation were another nine reports of pressurization problems directly attributed to the crews’ failure to set and verify the proper position of the pressurization mode selector to AUTO (Seven of these concerned Boeing 737 aircraft, while the other two events concerned McDonnell-Douglas aircraft). These nine reports all referred to aircraft that took off with the pressurization selector in inadvertently set to MAN (manual).
Source: Helenic Republic Accident Report, ¶1.18.2
- With respect to the Cabin Pressure Leak Test, the Ground Engineer simply recorded “Pressure run carried out to max diff” without making reference to the procedure/task number followed for this “pressure run.” According to the relevant AMM, Task 05-51-91-702-001, (entitled “Cabin Pressure Leak Test”), this test involved increasing the pressure in the aircraft “...until the differential pressure indicator shows a differential pressure of 4.0 psi.” At that time, the outflow valve was to be fully closed and, with the help of a stopwatch, the decrease in cabin differential pressure from 4.0 to 2.5 psi was to be plotted. To determine whether the leakage rate was acceptable, the plot was to be corrected using a correction factor curve which was provided in the same task description. Of particular importance is the fact that paragraph D (7) contained a note stating that “The indication on the differential indicator must not be more than 4.0 psi during a normal test” when increasing cabin pressure.
Source: Helenic Republic Accident Report, ¶2.2
The correct check would have been to bring the differential to 4.0 psi, fully close the outflow valve, and time the leakage. By simply demonstrating he could pump up the pressure to "max diff" the ground engineer did not prove anything at all about the leakage.
- . . . the Board noted the fact that the pressurization mode selector had been switched to MAN (manual) position in the course of the Cabin Pressure Leak Test. The condition of the pressurization system on the accident aircraft was evaluated based on the NVM data analysis at Nord-Micro. All these recordings indicated that the Digital Cabin Pressure Control System (DCPCS) was in the MAN (manual) mode, the Outflow Valve was constantly at 14,6 degrees opening angle (this was also the position the Outflow Valve Actuator was found at the accident site) and the flight mode was CLIMB. Cruise Flight Level was selected to 340 and Landing Field Elevation to 350 ft. The Cargo Heat Valve (Forward Outflow Valve) and both Pack Valves were indicated NOT CLOSED.
- All other messages are “030 INFLOW/LEAKAGE FAIL” which are recorded when the Outflow Valve is below 3 degrees opening angle for more than five consecutive seconds and therefore barely able to keep the cabin pressure on schedule. All these messages were recorded immediately after take-off and they have a number of occurrences during the same flight as shown by the intermittent count of four, i.e. there are four or more events. Both Pack-Valves are indicated open as well as the Cargo Heat Valve.
- All these messages indicated a continuous leakage situation with the aircraft that likely persisted for the last 74 flight legs. Only on the last flight is this situation not recorded, because the Outflow Valve did not modulate to compensate for the outflow of air, since the aircraft’s Cabin Pressure Controller Mode Selector had be left in the MAN (manual) position.
- Based on the above indubitable evidence, the Board concluded that the pressurization mode selector was in the MAN (manual) position from the time the aircraft was still on the ground.
- However, there was evidence that the flight crew had not performed their preflight duties as outlined in the relevant sections in the FCOM (see 1.17.2.2) in their entirety and/or correctly. When the aircraft departed, the pressurization mode selector remained in the MAN (manual) position (instead of AUTO) and remained there until the aircraft impacted the ground almost three hours later.
- Following takeoff, the flight crew was to perform an After Takeoff checklist, the first item of which was to check the pressurization system again and verify its settings. Although this checklist would have directed the flight crew’s attention to the pressurization panel, there was no evidence that the incorrect position of the pressurization mode selector was rectified.
- At an aircraft altitude of about 12 000 ft the cabin altitude warning horn sounded. Eight seconds later, the FDR showed the autopilot being disengaged, and re-engaged four seconds later. Eight seconds later, the FDR showed the auto-throttle being disengaged and the throttles retarded, but like the autopilot it also was re-engaged nine seconds later. Three seconds later, the No.2 radio was used to contact the Helios Airways Dispatcher.
- The Board examined the flight crew’s actions to disengage the autopilot and auto-throttle, and to retard the throttles upon onset of the warning horn. Given that the expected reaction to a cabin altitude warning horn would have been to stop the climb (there was no evidence to this effect), the Board considered such actions to signify that the flight crew reacted to the warning horn as if it had been a Takeoff Configuration Warning (the two failures use the same warning horn sound). This possibility was strengthened by the Helios Dispatcher who reported that when the Captain initially contacted him on the company frequency, he had referred to a takeoff configuration warning horn. This statement could not be verified because no voice transcript of this communication existed. Had the flight crew realized the significance of the warning horn, they should have immediately donned their oxygen masks, per the Operator’s Standard Operating Procedures.
- The Board concluded that the flight crew confused the two meanings of the warning horn. Similar occurrences had been reported by flight crews worldwide in the past. Given the benefit of hindsight, confusion of two meanings of one horn (one of which was designed to only sound when the aircraft was on the ground) appeared irrational.
Source: Helenic Republic Accident Report, ¶2.2
4
Cause
- During the Preflight procedure, the Before Start and the After Takeoff checklists completion, the flight crew did not recognize and correct the incorrect position of the pressurization mode selector (MAN position instead of AUTO).
- The green light indication that the pressurization mode selector was in MAN (manual) position should have been perceived by the flight crew during preflight, takeoff, and climb.
- At an aircraft altitude of 12 040 ft and at a cabin pressure that corresponds to an altitude of 10 000 ft, about 5 minutes after takeoff, the Cabin Altitude Warning horn sounded.
- The initial actions by the flight crew to disconnect the autopilot, to retard and then again advance the throttles, indicated that it interpreted the warning horn as a Takeoff Configuration Warning.
- The incorrect interpretation of the reason for the warning horn indicated that the flight crew was not aware of the inadequate pressurization of the aircraft.
- There were numerous remarks in the last five years by training and check pilots on file for the First Officer referring to checklist discipline and procedural (SOP) difficulties.
- The flight crew contacted the company Operations Centre Dispatcher and referred to a Takeoff Configuration Warning horn and the Equipment Cooling lights.
- Before hypoxia began to affect the flight crew’s performance, inadequate CRM contributed to the failure to diagnose the pressurization problem.
- The flight crew probably lost useful consciousness as a result of hypoxia some time after their last radio communication on the company frequency at 06:20:21 h, approximately 13 minutes after takeoff.
- Histological examinations revealed the presence of recent myocardial ischemia in both pilots, which according to the Hellenic Air Force Aviation Medical Centre (KAI) was likely due to the extended exposure to hypoxia.
- The toxicology test measured ethanol (34 mg/dl or 0.034 % weight/volume) in the specimen of the First Officer. The toxicological report stated that in view of the conditions, the finding may have resulted from post-mortem ethanol production.
- Shortly before flameout of the left engine, a member of the cabin crew was observed by an F-16 pilot to enter the flight deck, to sit at the captain’s seat, and to attempt to gain control of the aircraft.
- The above cabin crew member held a Commercial Pilot License.
- Non-recognition that the cabin pressurization mode selector was in the MAN (manual) position during the performance of the:
- Preflight procedure;
- Before Start checklist; and
- After Takeoff checklist.
- Non-identification of the warnings and the reasons for the activation of the warnings (cabin altitude warning horn, passenger oxygen masks deployment indication, Master Caution), and continuation of the climb.
- Incapacitation of the flight crew due to hypoxia, resulting in continuation of the flight via the flight management computer and the autopilot, depletion of the fuel and engine flameout, and impact of the aircraft with the ground.
Source: Helenic Republic Accident Report, ¶3.1
References
(Source material)
Hellenic Republic, Air Accident Investigation & Aviation Safety Board Aircraft Accident Report, Helios Airways Flight HCY522, Boeing 737-31S, at Grammatiko, Hellas, on 14 August 2005
Mayday: Ghost Plane, Cineflix, Episode 33, Season 4, 17 June 2007 (Helios 522)