This was the 10th of 13 Boeing 707s Pan American World Airways crashed and it would be easy to conclude it was just like the ten before it. In many ways, it was. As Robert Gandt put it in “Skygods,” his excellent book:
Another Pacific island. Another dark night, with rain and gusty winds, and yet another instrument approach to a runway without an electronic glide slope. A Pan Am 707 plowed through the jungle, short of the runway, then burned. Ninety-one people perished. By now it was clear to everyone, even the Skygods. The crash of Flight 806 on the island of Pago Pago brought to ten the number of Pan American 707s destroyed. Pan Am was littering the islands of the Pacific with the hulks of Boeing jetliners.
Gandt, p. 112
Updated:
2025-08-15

Pan Am 806 (Aircrash May Day)
This crash was on July 22, 1973. Ironically, Pan Am had just completed a sixty-nine page report three months earlier that each of the crashes was the result of human factors and what the report labeled, “substandard captains.” If you read the NTSB Aircraft Accident Report, you would come to that conclusion. But it was so much more than that.
Date: 30 January 1974
Time: 23:41
Type: Boeing 707-321B
Operator: Pan American World Airways
Registration: N454PA
Fatalities: 10 of 10 crew, 87 of 91 passengers
Aircraft fate: Damaged beyond repair
Phase: Approach
Airport (departure): Auckland International Airport (NZAA), New Zealand
Airport (arrival): Pago Pago International Airport, (NSTU) American Samoa
As I was taught during the Air Force Aircraft Mishap Investigation Course, accidents, mishaps, crashes, whatever you call them, are the result of human failures. It isn’t enough to say an engine failed, somebody caused the engine to fail. Maybe the pilot shut down the wrong engine. But it was more than just that pilot. Who trained the pilot? Who hired the pilot? Even something that seems obviously due to something not someone who failed, a someone is involved. A wing snaps off due to turbulence. Who allowed the aircraft into the turbulence? Who wrote the manual specifying what level of turbulence was acceptable? Who designed and certified the wing? In every case, a someone is to blame. Or, as with Pan Am 806, many someones are to blame. Let’s look at Pan Am 806 – the what – and the why.
3 — What happened: Fuel Planning
4 — What happened: The approach
5 — Why it happened: The airline wasn’t serious about pilot hiring, training, and checking
6 — What Happened: The survivable crash that wasn’t
7 — Why it happened: The airline wasn’t serious about HAZMAT
8 — Why it happened: The airline wasn’t serious about fuel tankering risks
9 — What happened – Boeing design: plug type, inward opening doors
10 — Why – Pan American: emergency exit instructions
11 — Why – Pan American: flight attendant training
12 — Why it happened – The ILS, a survivable windshear, and substandard pilots
1
What happened: A Prelude
As “Pan Am was littering the islands of the Pacific with the hulks of Boeing jetliners,” the Federal Aviation Administration took action:
Something was obviously wrong, and on April 27, 1974, a team of eight full-time investigators from the Federal Aviation Administration began an intensive inspection of Pan American’s operations.
For six weeks, with the willing cooperation of Pan Am staff, they turned the airline inside out. They flew on the routes and observed that 43 percent of crews were failing to carry out established cockpit procedures. They watched captains going through proficiency checks in the simulator, and while they were watching, 36.8 percent failed. They noted, ominously, that some of these would have passed by the examiners if the investigators had not been present.
“It is common gossip among the airmen, and in some cases cabin staff,” said the final report, “that Pan Am has captains and first officers that are considered substandard by their peers and have been carried by the company and need the help of strong co-pilots. Further, efforts were made by certain first officers, second officers, and flight engineers to specifically avoid having a flight schedule assignment, if at all possible, with some substandard captains.”
In other words, Pan Am was employing pilots with whom other pilots were scared to fly.
Norris, pp. 14 -15
This will be a factor in what follows.
2
What happened: HAZMAT
Clipper 806 had on board Hazardous Material (HAZMAT) in violation of known regulations.
The cargo in question was packaged by a local forwarding agent, Meadows Air Freight Ltd.
A Meadows clerk wrote out airwaybill number 026/3397 9525, describing the contents of the consignment as “Filler Catalyst – (non hazardas [sic]),” and had it delivered to the P.A. freight office at Aukland International Airport.”
It was only hours later that employees of Pan Am loaded the restricted material on board Clipper 806, soon bound for Pago Pago. MEK peroxide is not a “filler catalyst,” whatever that is supposed to mean.
Godson, p. 27
What is MEK? Methyl Ethyl Ketone peroxide, an alcohol, is highly explosive and regulations tightly control how it must be packed and limits the total quantity that can be transported aboard aircraft.
This will be a factor in what follows.
3
What happened: Fuel Planning
The NTSB report doesn’t mention the aircraft’s fuel other than to say it was within weight and balance. But the aircraft carried twice as much fuel as it needed for the trip:
There were 117,000 pounds of jet A-1 fuel aboard the aircraft upon departure from Aukland. The planned fuel burn-off for the flight to Pago Pago was 48.500 pounds. [ . . . ] The aircraft was carrying 37,900 pounds of stored fuel to be used on a later leg of the trip.
NTSB-AAR-77-7, Appendix C
This will be a factor in what follows.
4
What happened: The approach
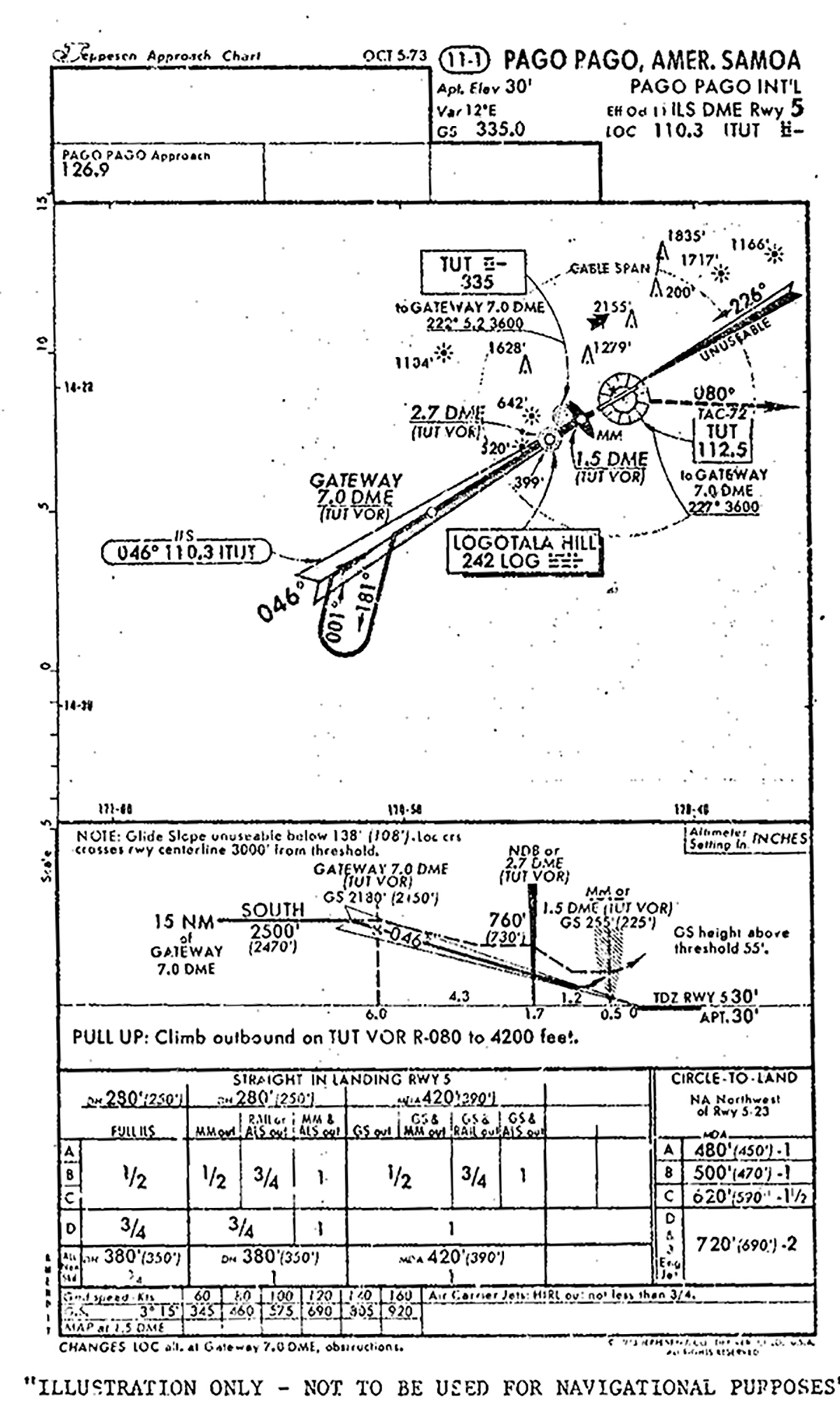
NTSB-AAR-77-7, Appendix D
The approach into Pago Pago wasn’t particularly difficult. Though it may seem complicated by today’s norms, the setup was fairly common back then. Clipper 806 reported its position 160 miles south of the airport and was cleared direct the Pago Pago VORTAC, to intercept the 20 mile arc, and then intercept the 226° radial of the VOR inbound. At that point they were cleared for the ILS DME Runway 5 approach by Pago Pago Approach Control. (There is no active control tower.) [NTSB-AAR-77-7, p. 2]
The CVR readout and the interview with the first officer established that the runway was in sight when the aircraft was about 8 nmi from the runway threshold. The runway probably remained in sight during most of the approach.
NTSB-AAR-77-7, p. 18
At this point, the captain’s instruments were set to the ILS and the first officer’s to the VOR to allow reference to the DME.
The aircraft descended about 500 ft. below the published minimum glide slope intercept altitude of 2,500 ft. before the glide slope intercept point was reached. [ . . .] The safety board was unable to determine the reason for this deviation from approach procedures.
NTSB-AAR-77-7, p. 18
In my opinion, the reason was apparent. More about that in the next section.
As the aircraft approached the glide slope, it continued through and above it as the captain started his descent. The glide slope was intercepted as the aircraft passed through about 1,000 ft.
NTSB-AAR-77-7, p. 19
Once again, the reason for this deviation will become apparent.
[Analysis] indicated that the aircraft encountered gusty wind conditions with a predominantly increasing headwind and/or an updraft about 50 seconds before impact. [ . . . ] The windshear was evident by a sharp increase in airspeed and a shallowing of the descent path. Consequently, the aircraft went above the glide slope. [ . . . ] The sound spectrogram showed that at this time, the thrust was reduced to apparently correct the high and fast condition.
As the aircraft passed Logotala Hill, it apparently came out of the increasing headwind or updraft condition and the positive performance effect was lost. In fact, a wind which produced a small negative performance effect was probably encountered. The thrust was well below that normally needed for a stabilized approach and about 16 seconds before impact, the aircraft started a rapid descent of about 1,500 fpm.
Thus, the Board concludes that the captain recognized the initial effect of the windshear condition and acted to correct the aircraft’s flight profile by reducing thrust, but he did not recognize the second effect as the windshear condition changed. Consequently, the aircraft, with low thrust, responded to the changing wind by developing a high descent rate. The captain had at least 12 seconds in which he could have taken action to arrest the descent in time to prevent the accident. During that time, the total thrust available exceeded that required to maintain constant airspeed in level flight. That the necessary pitch attitude and thrust changes were not applied can only indicate that the flightcrew was not aware of the high descent rate and the impending crash.
Evidence indicated that when the sink rate increased, the captain may have been looking outside the aircraft and therefore was not flying by reference to the flight instruments. At the time the sink rate increased to about 1,500 fpm, the aircraft was over an area devoid of lights (known as a “blackhole”), a heavy tropical rainstorm was over the airport and moving toward the approach end of the runway, and the first officer had called the runway in sight.
NTSB-AAR-77-7, pp. 19 – 20
The only callouts made were by the first officer.
At 2340:22.5, the first officer stated, “You’re a little high.” [ . . . ]
From 23:40:29.5 to 23:40:34, the radio altimeter warning tone sounded twice. At 2340:33.5, the first officer interrupted the second warning tone with, “You’re at minimums.”
As 2340:35, the first officer reported, “Field in sight.” Seconds later, the first officer stated, “turn to your right,” followed by “hundred and forty knots.” This was the last communication reported on the CVR.
NTSB-AAR-77-7, p. 3
The “turn to your right” call would have been normal, as the ILS was offset in heading from the runway.
At 2340:42, the aircraft crashed into trees at an elevation of 113 feet, about 3,862 feet short of the runway threshold.
NTSB-AAR-77-7, p. 3
When this crash occurred, in 1974, our awareness of windshear wasn’t what it is today. The event that really shaped that awareness was Eastern Air Lines Flight 66 in New York-John F. Kennedy International Airport, NY (JFK, KJFK), a year and a half later. But as the NTSB report points out, we were aware of windshear and the need to monitor vertical speed on approach. As they pointed out, once the “gain shear” left them above glide path and with the throttles retarded, the crew should have been ready to add thrust as the aircraft returned to glide path. But they didn’t. Why?
5
Why it happened: The airline wasn’t serious about pilot hiring, training, and checking
At the time of Clipper 806, Pan American World Airways was experiencing a wakeup call and making the initial steps of getting its house in order. Decades of hiring the wrong kinds of pilots, however, would take more than just a wakeup call to fix. The pilots on Clipper 806 were not the airlines’ finest.
Captain Leroy Petersen had been off flying status for four months for medical reasons and cleared for flight after “voluntary simulator training” after which it was said, “by the end of the period, Captain Peterson was doing very good work.” The NTSB report leaves his capabilities at that, neglecting to mention:
He passed these tests, but the flight section was carried out in daylight under visual meteorological conditions.
Norris, p. 20
In this book, “Willful Misconduct,” William Norris finds out, “what kind of pilot was in charge of Flight 806” by examining his training records:
December 20, 1951: Thinking and judgment of a professional and intelligent airmen were marginal.
July 2, 1957: ILS work with the ZR [navigation instrument] very poor.
August 29, 1963: Repeated four-engine ILS approach too fast [ . . .] over-control on ailerons caused vertical bar excursions.
June 1, 1965: Failed FAA oral exam for 707 type rating.
June 21, 1965: Failed FAA flight portion of the exam required for issuance of a Boeing 707-20 rating. Unsatisfactory landing technique.
June 25, 1965: Failed re-check for FAA 707-20 rating.
June 26, 1965: Three-engine ILS missed approach was very weak.
October 16, 1965: Heading control not precise. Over-control of elevator and throttles on ILS, introducing yaw and roll.
December 21, 1972: Repeated three-engine ILS for glide-slope tracking.
June 28, 1973: We had to repeat three-engine ILS, due to being out of limits at decision height.
Norris, pp. 21 – 24
Norris concludes:
Captain Petersen was a man who had trouble with instrument landings, and he had suffered this deficiency throughout his career.
Norris, p. 24
Petersen was accompanied by First Officer Richard Gaines, who was suffering from laryngitis and gave up his seat to Second Officer James Phillips. Phillips’ training record wasn’t inspiring:
June 6, 1966: Student a little slow. Knows procedures but hesitates to make corrections.
August 21, 1966: Student unable to execute ILS due to slow scan resulting in poor airspeed control. Did not stay on either glideslope or localizer within prescribed minimums.
August 23, 1966: Quite a bit behind the aircraft throughout.
August 15, 1967: Lack of thinking is still causing difficulty.
November 12, 1968: Slow following approach procedure.
Norris, pp. 25 - 26
But even had Gaines been able to sit in the right seat, things may not have been any better:
September 22, 1964: Slow reaction to corrections on power. Airspeed and heading control slow.
October 20, 1964: Instrument scanning a little slow.
April 27, 1965: Slow scanning and erratic altitude control.
November 30, 1965: Altitude control was ragged, and there was little or no use of vertical speed.
December 18, 1966: He is unable to see objective of minima.
December 23, 1966: Due to the unsatisfactory rating he received on many items, it is recommended that the type rating training be discontinued.
May 8, 1967: This pilot is slow and indecisive about almost everything he does.
Norris, pp. 28 – 30
You can’t have been a professional pilot for long without a comment or two like these in your training record, but all three pilots seem to have more than their share.
6
What Happened: The survivable crash that wasn’t
The aircraft continued through the jungle vegetation, struck a 3-foot-high lava rock wall, and stopped about 3,096 feet from the runway threshold. The aircraft was destroyed by impact and the subsequent fire.
NTSB-AAR-77-7, p. 3
The terrain in the area of the crash sloped down gently about 3.5 degrees and while the aircraft’s engines and much of its wings were torn off, the cabin area in the fuselage was mostly intact.
Passengers who survived the accident said that the impact forces were slightly more severe than a normal landing. No damage to the cabin interior was reported. Large fires were seen outside the right side of the aircraft. One person opened an overwing exit on the right side of the aircraft; flames came in through the exit, and he closed it. Other survivors opened the left overwing exits, and all the survivors except the first officer escaped through these exits.
NTSB-AAR-77-7, p. 11
The first officer escaped through a hole in the cockpit. So this leaves a question: what about the left forward and aft exits?
Postaccident investigation revealed that the forward and the rear entry doors were not opened or used for escape. The forward door was opened about 2 to 3 inches, but the aft door was closed.
NTSB-AAR-77-7, p. 11
The report concludes:
The injuries sustained by the fatally injured passengers as well as the surviving passengers were direct results of the post crash fire.
NTSB-AAR-77-7, p. 27
So, we are left with two questions: why didn’t the passengers escape through the left forward and aft entry doors and why was the fire so intense? The NTSB report seems reluctant to speculate, but does offer a few facts.
7
Why it happened: The airline wasn’t serious about HAZMAT
The aircraft was carrying restricted cargo. The cargo, listed as article No. 727 by the International Air Transport Association (IATA) Restricted Articles Regulation, was methyl ketone peroxide (MEK peroxide). IATA regulations specify the maximum quantity that may be packed in any one outside container is ½ kilogram (1 pound) or ½ litre (1 pint). . . . The weight of the MEK peroxide in the cartoon was 4 kilograms.
NTSB-AAR-77-7, p. 15
We often talk about the massive team effort needed to safely fly an airplane from Point A to Point B, but not often enough about the team needed to load the airplane’s cargo and luggage so as to not endanger the flight.
Pan Am had a recent history of violating Hazardous Material (HAZMAT) rules and lost a Boeing 707 just eighty-eight days before Flight 806. The all-cargo Pan American Flight 160 had departed New York-John F. Kennedy International Airport, bound for Glasgow-Prestwick Airport, United Kingdom. Shortly after takeoff, improperly packed acid leaked onto saw dust packing material. The resulting smoke caused the crew to divert to Boston, but they had inadvertently deactivated the yaw damper which led to the loss of control of the aircraft. All three onboard were killed.
You could argue that the industry itself wasn’t serious enough about HAZMAT, placing the responsibility on the airline to make sure anything that showed up as cargo was properly labeled and packaged. That is probably a valid point. We’ve gotten better since Clipper 806, but as ValuJet Airlines Flight 592 (https://code7700.com/case_study_valujet_592.htm) in 1996 and UPS Airlines Flight 6 (https://code7700.com/case_study_ups_6.htm) in 2010 demonstrated, we have more to learn about the dangers of flying with HAZMAT.
While the NTSB Report makes note of the presence of unauthorized HAZMAT onboard the aircraft, it does not tie it to the post-crash survivability. In my opinion, it isn’t unreasonable to speculate that the MEK could have increased the intensity of the fire, the resulting smoke, and combined these could have been a factor in elevating passenger panic.
8
Why it happened: The airline wasn’t serious about fuel tankering risks
Though the NTSB report is silent on the issue of fuel tankering, it became an issue during post-crash law suits:
Though its passenger load was well below capacity, the Boeing 707-321B sat heavy on the tarmac at Aukland on that late summer evening. Of its gross weight, 40 percent consisted of 52.3 tons of A1 jet fuel. [ . . . ] There was nothing unusual about this for a Pan American aircraft at this moment in history. It was all part of the company’s economy drive. During the oil crisis, fuel was in short supply and more expensive at some airfields than at other. It was Pan American policy to pick up excess fuel at the cheaper locations, so that less would be needed when the aircraft landed at more expensive points.
Norris, pp. 18 – 19
In my opinion, the airline should have weighed the advantages of fuel tankering against the impact on approach speeds and the possibility of making any crashes less survivable. As most aviators know, “it costs fuel to carry fuel,” and in the Boeing 707, it is doubtful the tankering actually saved money at all.
9
What happened – Boeing design: plug type, inward opening doors
A Boeing 707 plug door operates with a unique mechanism designed to ensure a strong seal against the fuselage by using the pressure difference between the inside and outside of the aircraft.
The door is larger than the opening it fits into, so it cannot simply swing outward. To open, the door first moves inward slightly into the cabin. This inward movement allows the door to clear the frame because the door's dimensions are wider than the opening. This is similar to pulling a plug inward before it can be removed, which is why it's called a "plug door".
After moving inward, the door rotates on an axis (or sometimes two axes) inside the door frame. This rotation aligns the door so it can then slide or swing outward, parallel to the fuselage. The door hinges and mechanisms are designed to allow this complex movement—first tipping or swinging inward, then rotating, and finally moving outside the aircraft. The operator doesn’t need to know anything other than you have to pull the door in before pushing it out.
This might seem like putting a square peg into a round hole, but it works because of the door’s geometry. The best explanation I’ve seen is in this short YouTube video: YouTube Aircraft Plug Type Doors B747 Demonstration.
When the aircraft is pressurized, the higher pressure inside pushes the door outward into its frame, creating a tight seal that prevents it from being opened during flight. The pressure essentially "plugs" the door in place. This means the door cannot be opened outward until the pressure inside the cabin is equalized with the outside pressure. This design ensures safety by making it physically impossible to open the door at altitude without equalizing pressure first.
The key point during an emergency egress is that the door must be pulled inward before it can be pushed out.
10
Why – Pan American: emergency exit instructions
One of the books about Pan Am 806 makes a point about the passenger information cards, closing the book with the point the cards were wrong.
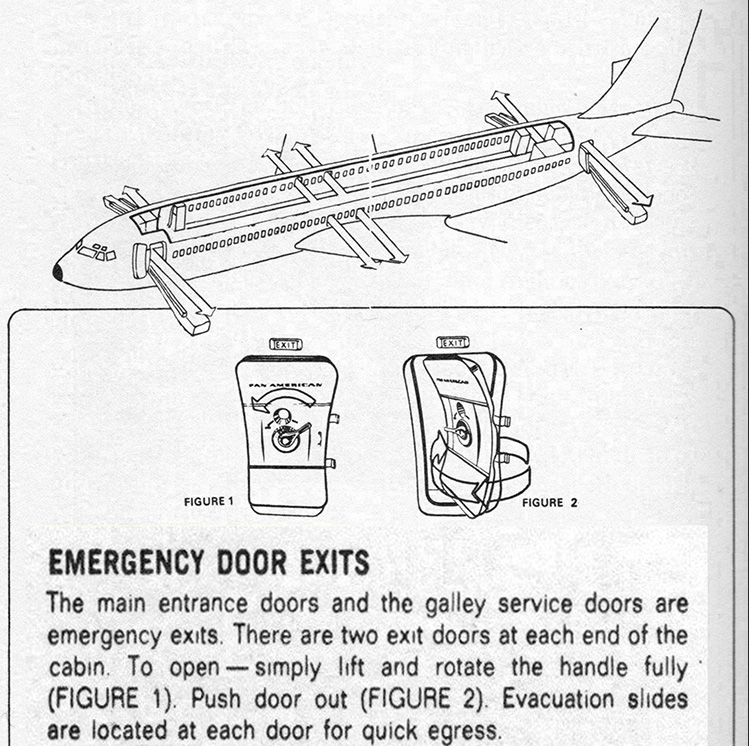
Emergency Instructions, Pan Am Boeing 707 (Extracted), Godson, p. 204
The instructions say “push door out” and neglect to say the first move is to pull the door in. The NTSB report doesn’t mention this at all, but I think these instructions may not have been a factor at all. Consider, for example, how these instructions appear on a modern Boeing passenger jet:
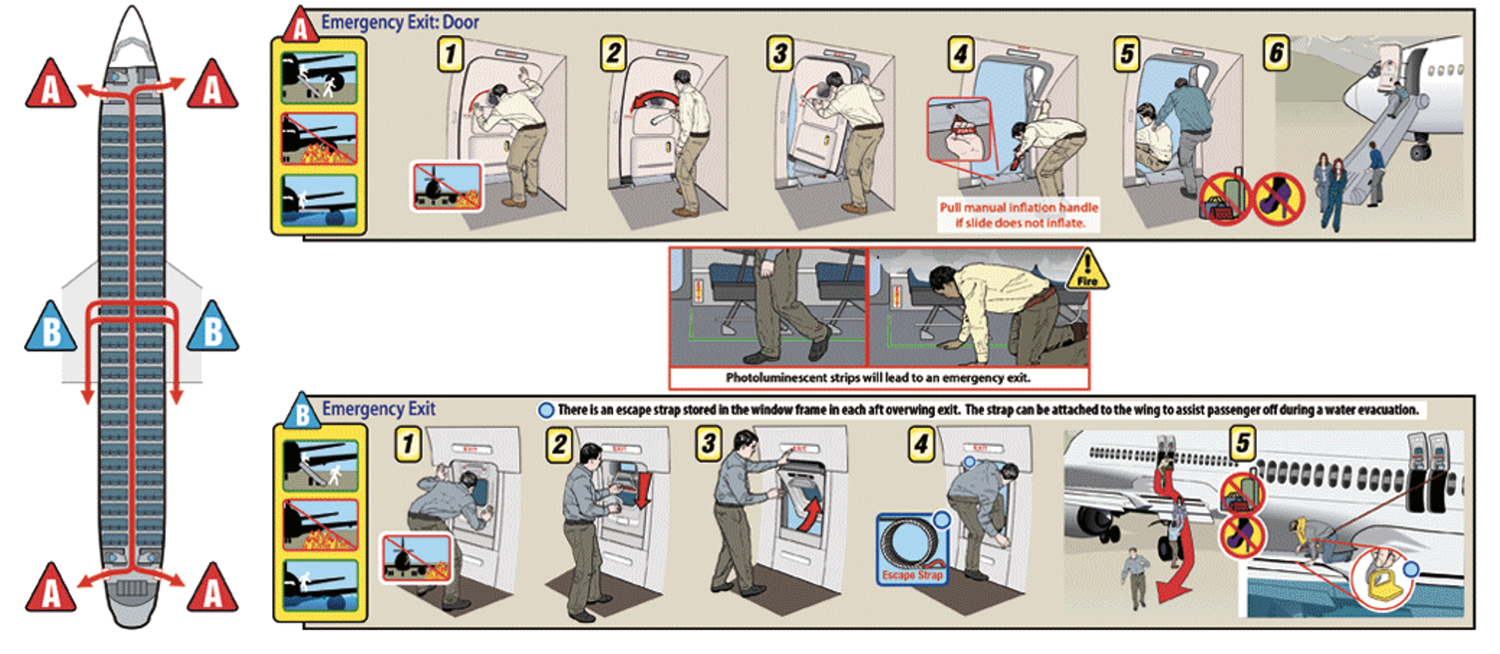
Boeing 737 example emergency door instructions
I’ve operated a similar door in the Boeing 747 and the door itself makes the initial inward movement when you rotate the handle. In any case, the door is not meant to be operated by passengers.
11
Why – Pan American: flight attendant training
The book by Godson goes to great lengths to cite the problem with the passenger information cards and the error on those cards saying the cabin doors must be pushed out, neglecting to say they must first be pulled in. The cards are wrong, but I’m not sure how much of a factor they were. But Godson does point out the problem that interests me more:
Then why were NONE of the doors used?
Taking into account the limited details available and speculating on what must have happened inside Clipper 806’s cabin, there seems to be only one possible conclusion.
Remembering that it takes a properly trained person only a few seconds to move a Boeing 707 door from a “closed and locked” to a “fully open” position, there was plenty of time for those on board to deploy, at the very least, SOME of the four doors had they acted quickly enough.
Of the four, the only one remaining after the fire was on the front left-hand side. The investigators found it dangling, partly opened, on its hinges. Firemen and others all confirmed that the door was unlocked, but it was not FULLY opened. The rescuers discovered more than twenty bodies neatly stacked one on top of the other in the immediate vicinity of this egress.
Since NONE of the crew’s corpses was found near the doors, what more than likely happened was that as the Clipper slid through the jungle undergrowth, panic-stricken passengers left their seats and headed for the main exits, both at the front and the rear of the plane. [ . . .] The cabin staff did not take part in this premature escape attempt. Moreover, two stewardesses’ bodies were found well away from the rear main door. Why they did not lead or at least help with as escape, nobody knows.
[ . . . ]
The facts are that the passengers were at the exits before the more than likely completely inactive crew. There was a general panic when difficulty was experienced in getting them opened.
[ . . . ]
If you know what you are doing, unclosing the exits of a Boeing 707 is really not that problematical. They are “plug-type” in operation. All that has to be done, once the locking handle has been turned, is to PULL THE DOOR INSIDE – the exact opposite of what the printed emergency instructions say is to be done.
Godson, pp. 211 - 213.
The problem that may have really shaped the outcome is the “completely inactive crew.” Survivors stated that some of the passengers started moving to the exits while the aircraft was still in motion after it impacted the ground. In my opinion, flight attendants need to proactively and aggressively control the cabin in an emergency situation. “Remain seated!” Block the aisle, make eye contact, and force a panicking passenger to either physically push you or back down.
None of this is to say the flight attendants were causal to the crash itself, but they could have been instrumental in the post-crash survival. The cause of the crash itself, no doubt, was the pilots up front.
12
Why it happened – The ILS, a survivable windshear, and substandard pilots
At the time, much of the news focused on the wind shear and the so-called “black hole approach.” During the trial that followed the crash, the most crucial witness was retired Pan Am Captain Charles Basset, who had flown for the airline since 1940, twenty-three of those as a check airman and the most recent ten as a Boeing 707 captain.
“Do you have an opinion as to whether or not the flight crew of Flight 806 acted in a manner consistent with Pan American’s operating procedures?”
“No,” Bassett replied firmly. “They did not.”
Did he consider the approach to Pago Pago at night a black hole?
It was not a black hole to Captain Bassett, and he proceeded to blow the theory apart. It simply did not matter whether there were lights on the ground along the approach path or not, he said, because right down to the decision height of 280 feet the captain would be flying on his instruments, not looking outside. When he raised his eyes, he would have the runway lights in front of him. So much for the black hole.
[ . . . ] He went on to itemize the errors:
• The rate of descent had exceeded 1,000 feet per minute. There should have been a warning call at 900 feet per minute and there was not.
• There should have been a callout at 100 feet above decision height. There was not. Nor was there a call at 500 feet above the ground.
• The speed of the aircraft, which should have been stabilized at 150 knots from a point some seven miles out, had gone up to 180 and perhaps 190 knots inbound from Logotala Hill.
• The flaps should have been put down at the intersection of the glide slope, and it had not been done.
Norris, pp. 251 - 252
13
Conclusions
The NTSB report’s conclusions focus on what happened and not why. The statement of probable cause follows this pattern:
The National Transportation Safety Board determines that the probable cause of the accident was the flightcrew's late recognition and failure to correct in a timely manner an excessive descent rate which developed as a result of the aircraft's penetration through destabilizing wind changes. The winds consisted of horizontal and vertical components produced by a heavy rainstorm and influenced by uneven terrain close to the aircraft's approach path. The captain's recognition was hampered by restricted visibility, the illusory effects of a "blackhole" approach, inadequate monitoring of flight instruments, and the failure of the crew to callout descent rate during the last 15 seconds of flight.
NTSB-AAR-77-7, p. 15
Why investigate an aircraft accident and publish any report at all? The answer should be to prevent recurrence of the accident. I would write the report’s probable cause as follows:
- The Federal Aviation Administration failed to properly oversee Pan American World Airways’ pilot hiring, training, and checking, as well as the airline’s flight operations.
- The National Transportation Safety Board failed to adequately investigate the ten previous Pan American World Airways accidents, many of which demonstrated identical pilot issues, and follow through with the FAA and the airline.
- Pan American World Airways failed to hire competent pilots.
- Pan American World Airways failed to train its pilots in instrument flight procedures and crew resource management techniques.
- Pan American World Airways failed to implement and enforce a robust Hazardous Materials program.
- Pan American World Airways failed to train its flight attendants adequately for emergency procedure situations.
- The pilots of Flight 860 failed to properly fly the ILS.
- The flight attendants failed to control the cabin after the initial impact.
References
(Source material)
Godson, John, Clipper 806: The Anatomy of an Air Disaster, Contemporary Books, Inc., Chicago, Illinois, 1978.
Norris, William, Willful Misconduct: The Tragic Story of Pan American Flight 806, CamCat Publishing, LLC, Brentwood, Tennessee, 2020.
NTSB-AAR-77-7, Aircraft Accident Report – Pan American World Airways, Inc., Boeing 707-3125, N454A, Pago Pago, American Samoa, January 30, 1974, National Transportation Safety Board, Washington, D.C., 6 Oct 77