I am posting this case study fifty years to the day after Trans International Airlines Flight 863 took off from KJFK with crew only, scheduled to fly to KIAD to pick up passengers on their way to London. A lot has changed in those five decades and most operators and pilots have fully absorbed the lessons from this crash. I worry that some pilots, young and old, might not have witnessed just how dangerous the simply mundane can be. This is a good one to reinforce that no details are too small to consider in aviation.
— James Albright
Updated:
2020-09-08

DC-8 N4863T (Steve Aubury)
On the surface of the event is the thought that a bit of asphalt got kicked into the elevator and caused the airplane to rotate early and eventually takeoff in an uncontrolled manner. As the NTSB points out, once the airplane was airborne there was very little the crew could have done. The DC-8 was built with control tabs, much like the balance tabs used in Boeings of the era, in some of the flight controls and the gaps between surfaces may have made it more susceptible to this kind of Foreign Object Damage (FOD). So two things to do, back in 1970. First, design better flight control systems, less susceptible to this kind of thing. Second, do a better job of keeping the areas near airplanes FOD free. Okay, job done. Or is it?
A closer reading of the NTSB report reveals that when the airplane rotated prematurely, the aircraft had only used 1,500 feet of the runway. The airplane then dragged its tail on that runway for nine seconds before lifting off. The mindset back then was about the only thing worthy of a takeoff abort was an engine failure or fire. But picture yourself with the tail dragging on the runway, you are just doing 100 knots, you have most of the runway in front of you, and you don't know why the nose isn't reacting to your full nose down elevator movement on the yoke. Wouldn't that be worth an abort? The report never mentions V1 but part of my "go / no-go" briefing includes "if the airplane will not fly" as a valid reason for an abort above V1. Left unsaid but implied, "if the airplane will not fly under my control."
Here are the lessons as I see them:
- FOD
- Flight Control Checks
- First Officer Abort Authority
Earlier this year I landed at a small Florida airport I had never been to but certainly large enough for my Gulfstream. I was shocked by the condition of the taxiways and ramp and even more disheartened by all the loose gravel. I was fortunate to have three mechanics on board (this was a maintenance proving run) who inspected the airplane from nose to tail and gave us a clean bill of health. The next day we fired up and left. In retrospect, I should have had the airplane towed to someplace devoid of these threats before firing up and leaving. We all make mistakes and this was one of my bigger ones.
This crew did a flight control check during their taxi to the runway but apparently the errant piece of pavement was kicked to their tail after this. The Gulfstream world has adopted a last minute flight control check just prior to taking the runway. At first I thought this was overkill — I did a flight control check after engine start in the chocks, after all — but now I understand the wisdom of this technique.
The NTSB report dances lightly on the subject in this accident. It was the first officer's takeoff and he only commented that he could not control the aircraft after they were airborne. I suspect he realized this well before but deferred to the captain's judgment. I think if the first officer realizes the aircraft will not fly under his or her control, he or she should abort the takeoff and sort out the details later.
1
Accident report
- Date: 8 September 1970
- Time: 16:06
- Type: McDonnell Douglas DC-8-63CF
- Operator: Trans International Airlines
- Registration: N4863T
- Fatalities: 11 of 11 crew, 0 of 0 passengers
- Aircraft Fate: Destroyed
- Phase: Takeoff
- Airport: (Departure) New York-John F. Kennedy International Airport, NY (KJFK)
- Airport: (Destination) Washington-Dulles International Airport, DC (KIAD)
2
Narrative
- Trans International Airlines (TIA) Ferry Flight 863, a Douglas DC-8-63F, was engaged in a ferry flight from J. F. Kennedy International Airport to Dulles International Airport, Washington, D. C., where passengers were to board for a flight from Washington to Gatwick International Airport, London, England.
- At 1604, Flight 863 was cleared into takeoff position, with instructions to hold and, at 1604:55, the flight was cleared for an immediate takeoff.
- Based on information from the Cockpit Voice Recorder (CVR) and the Flight Data Recorder (FDR), the takeoff roll began at 1605:07, and the tail skid began dragging on the runway at 91 knots (the computed rotation speed was 124 knots), 1,550 feet from the takeoff end of the runway, at 1605:26, The tail skid dragged on the runway intermittently for an additional 1,250 feet.
- At 1605:35, when the aircraft was about 2,800 feet down the runway, the aircraft became airborne and, according to pilot-qualified witnesses, rotated slowly to an unusually nose-high attitude. Stall warnings (Stick shaker) were recorded on the CVR within l to 2 seconds after lift-off and continued until 1605:49. Witnesses stated that the aircraft reached a nose-high attitude estimated to be between 60° and 90° at an altitude of 300 to 500 feet above the ground. The aircraft then rolled about 20° to the right, rolled back to the left until the left wing was approximately perpendicular to the ground, and descended in a left-wing-down, nose down attitude. The aircraft contacted the ground at 1605:52, on its left wing and the nose. The wreckage was immediately engulfed in flames. The crash firefighting crew arrived at the wreckage approximately 30 seconds after the accident, and brought the fire under control in about 5 minutes.
Source: NTSB-AAR-71-12, ¶1.1
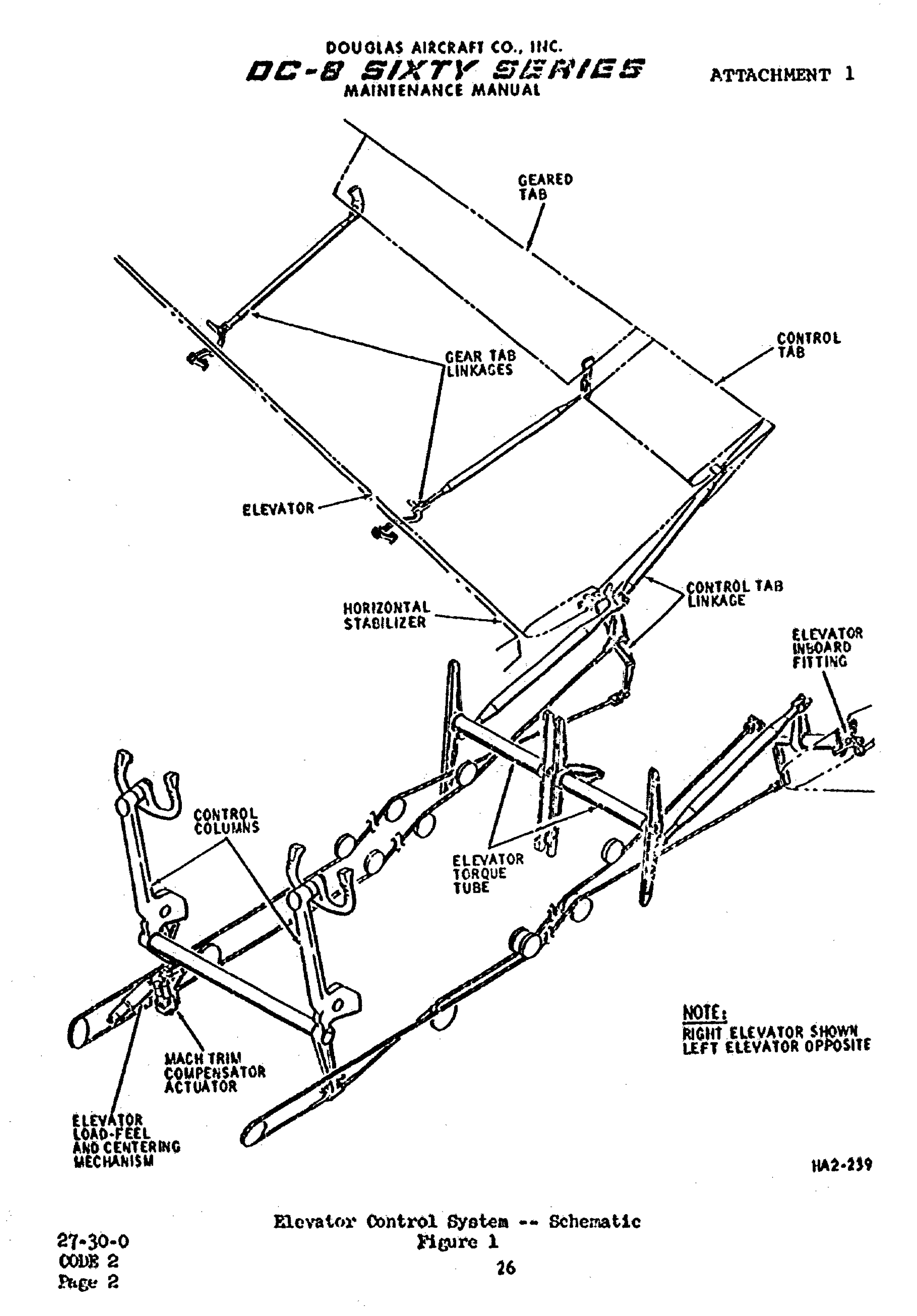
Elevator control system, NTSB-AAR-71-12. figure 1.
- The elevator control system of the DC-8 Sixty Series aircraft is actuated mechanically and consists of elevators, control tabs, geared tabs, control columns, a load-feel and centering mechanism, and elevator dampers.
- The elevators are operated aerodynamically by the tabs which are controlled by a cable system from the control column. The geared tab on each elevator is linked mechanically to the stabilizer so that as the elevator moves, the geared tab moves in the same direction as the control tab to provide additional aerodynamic control surface.
- The elevators are hinged to brackets attached to the horizontal stabilizer rear spar. Elevator travel is approximately 27° trailing edge up (TEU) and 16-1/2° trailing edge down (TED) from the neutral position. The elevators are interconnected by a torque tube so they can operate in unison. Both elevators are aerodynamically balanced and mass balance weights are installed in the leading edge to minimize flutter. The mass balance causes the elevator to be in the approximate 27° TEU position when no aerodynamic load is applied and the gust locks are disengaged.
- If the control column is pulled aft from this static position, the elevator remains fixed as the tab moves from full trailing edge up to full trailing edge down. If the control column is pushed forward from the static position, the control tab remains fixed as the elevator moves from the full trailing edge-up position to a trailing edge-down position.
- When the control column is moved forward or aft in flight, the cable system and mechanical linkage cause the elevator tabs to move up or down and, during flight, aerodynamic forces on displaced tabs drive the elevators. As the position of the elevators changes in relation to the horizontal stabilizer, mechanical linkage moves the geared tabs so as to provide additional aerodynamic boost to assist in moving the elevators.
- The TIA DC-8 Flight Operation Manual required pilots to test the flight controls to the full limits of their travel prior to takeoff. Movement of the controls was to be accomplished slowly and smoothly to avoid damage to boosted controls (rudder and ailerons). The CVR transcript indicated that the flight controls were checked while the crew was taxiing to the runway.
Source: NTSB-AAR-71-12, ¶1.6
The accident occurred in bright daylight.
- JFK Airport had been undergoing an expansion and modernization program including the relocation of the outer and inner taxiways and ramp expansion. This work required the removal of old paved surfaces and resulted in taxiway and runway contamination.
- Introduction of the new large jet aircraft with more than twice the thrust of previous jet (transport) aircraft, caused considerable erosion along most taxiways and runways. According to New York Port Authority personnel, the products of this erosion, pieces of asphaltic material, rocks, etc., were being blown onto taxiways, ramps, and runways, making it difficult to keep these areas clean.
Source: NTSB-AAR-71-12, ¶1.7
- The horizontal stabilizer trim setting was 2° aircraft nose up, approximately the correct setting for takeoff at the calculated weight and center of gravity.
- The landing flaps were extended to 23°, the takeoff position.
- The gust locks showed no evidence of being engaged.
- During the examination of the right horizontal stabilizer, a hole was found in a rear spar web access door at approximately stabilizer Station 32, This hole appeared to have been punched in the access door by a foreign object. On that portion of the leading edge of the right elevator that faced the hole, an area of scratches and gouges was found. There were scratches adjacent to and below the hole in the access door and a smear of asphaltic material adhered to the metal near the hole.
- No foreign object was found in the stabilizer or in the area between the elevator and the stabilizer. However, several tar-covered stones, 1-1/2 to 2 inches in diameter, were found in the vicinity of the empennage.
Source: NTSB-AAR-71-12, ¶1.12
3
Analysis
- Examination of the horizontal stabilizer established that it was in a position appropriate for the takeoff conditions. The landing flaps were positioned properly at the takeoff setting. There was no evidence of structural or system malfunction of the pitch control system. The elevator torque tube bearings and elevator hinges that were examined showed no evidence of prior distress.
- Calculations performed by NTSB and the manufacturer indicate that, given the takeoff conditions, 16° of elevator trailing-edge-up deflection (aircraft nose up) would have been sufficient to perform the initial rotation at an airspeed of approximately 80 knots. The correlation of the cockpit voice recorder record, the flight data recorder record, and the witness observations indicated that the aircraft had rotated to an excessively nose-high attitude at an indicated airspeed of approximately 91 knots at a point approximately 1,500 feet past the beginning of the takeoff roll. The initial elevator deflection was not maintained throughout the flight. These studies also indicated that the aircraft was capable of performing the maneuvers described by the witnesses but that the elevator angle would have gradually decreased throughout portions of the flight.
- Physical evidence that could be associated with a pitch system problem was the position of the elevator, the discovery of the hole punched in the right horizontal spar web access door, the scarring of the opposite corresponding area on the leading edge of the right elevator, and traces of asphaltic materials found around the periphery of the hole in the access door. This evidence, coupled with the discovery of several large, asphalt-covered stones in the area of the recovered tail section, led the Board to test the effect of lodging a similar size stone in the area between the leading edge of the elevator and the trailing edge of the stabilizer. When a stone was so placed in this area and the elevator moved to the aircraft nose up position, the stone followed the leading edge of the elevator down into the space between the elevator and the stabilizer. When force was applied to the elevator to return it to the level position, the stone jammed into the space and kept the elevator from moving. As more force was applied to move the elevator down, the metal was seen flexing and buckling where the stone pressed on it.
- Calculations based on an ultimate shear failure mode were provided by the manufacturer. These calculations indicated that the loads required to fail the material in the access door varied according to the length of the contact line between the foreign object and the door. For example, if the contact line were 1 inch long, 1,720 pounds would have been required to achieve the ultimate shear value of 43,000 p.s.i.; however, if the contact line were only .5-inch long, the load would be reduced to 860 pounds to achieve the same ultimate shear value.
- Examination of the leading edge of the right elevator and the trailing face of the right stabilizer indicated that an irregular shaped, asphalt-covered, hard object was lodged between the two surfaces. Calculations based on the fresh scars and marks in this area indicated that the elevator was approximately 12° trailing edge up when sufficient force was applied to cause the foreign object to scar and pit the metal. Scrape marks on the access door indicated that the object skidded or slid, under pressure, up the face of the door. Finally, the object punched an irregular hole in the door and then fell free, probably upon impact.
- The Board believes that this foreign object was a stone similar to the ones found in the accident area. Similar stones were also found on nearly all the taxiways and aprons used by Flight 863 prior to takeoff. These stones were lying loose on the surface of the airport during the resurfacing program in progress at the time of the accident. While the Port Authority continuously swept the taxiways and runways, they were unable to keep up with the requirements for removal of debris from all the paved areas. Jet blasts associated with normal operations, particularly those generated by aircraft with more than average thrust, were observed blowing similar stones over the surface of the airport.
- After reviewing the evidence, the Board believes that the loss of pitch control was caused by a foreign object lodged between the right horizontal stabilizer and the leading edge of the right elevator. The object could have been thrown into that position by jet wake during taxiing or runup. With the object lying in the area between the surfaces, displacement of the elevator to the trailing-edge-up position would have allowed the object to fall between the two surfaces. In view of the static deflection of the elevator in this type of aircraft, trailing edge up, any time the flight controls were unlocked the elevator would assume that position and create a gap between the elevator and the stabilizer. A large deflection of the elevator was also observed during the initial takeoff roll of other DC-8's in normal operation.
- As the takeoff of N4863T was initiated, the air load on the deflected elevator would have built up, increasing the pressure on the object by attempting to streamline the elevator. The compression of the object between the surfaces could have caused the pitting and scarring of the surfaces that was found.
- At approximately 80 knots, an abnormally low airspeed, the aircraft began to rotate, and at approximately 91 knots, the tall skid struck the runway. As the airspeed increased and the pilots increased the nose down input, the load on the object caused it to move toward the top of the control surfaces and caused the scratches observed on the access door below the puncture. At the same time, the elevator angle was decreasing toward the 12° position. At approximately that point, a sharp edge or point of the object penetrated the skin of the access door and jammed the elevator in that position. As the load on the elevator increased, the elevator up angle was further reduced to an estimated value of 5° to 8°. The restriction to elevator movement was not detected by the crew in time to successfully reject the takeoff.
- The evidence indicates that a strong push force was applied to the control column. Additionally, a relatively small amount of forward trim, aircraft nose down, was used. The amount of trim was only about one-half of a degree, however. Finally, there was a recorded verbal indication by the first officer that he could no longer control the aircraft. This statement was not made until after the aircraft had left the ground.
- As the aircraft began to rotate, at a speed of approximately 80 knots, this should have been the first indication to the crew of an abnormal condition. About 4 seconds later, at 91 knots, the tail skid began to drag on the runway and continued to do so for approximately 9 seconds. The aircraft subsequently became airborne at an airspeed of approximately 117 knots and immediately resumed its upward rotation. At this point, there was no other reasonable alternative available to the crew than to continue the takeoff; and the accident became inevitable.
- There should have been ample time for the pilots to recognize the abnormal behavior of the aircraft, i.e., early rotation and dragging of the tail skid, and under such circumstances the takeoff should have been rejected. The captain, even though he was outside the control loop, should have immediately recognized an abnormal condition and, without having to know the precise reason for the abnormality, should have either taken control or ordered the takeoff rejected. The first officer, being part of the control loop, should have recognized an abnormal condition when appropriate control inputs did not correct the premature rotation of the aircraft.
Source: NTSB-AAR-71-12, ¶2.1
4
Cause
The Board determines that the probable cause of this accident was a loss of pitch control caused by the entrapment of a pointed, asphalt-covered object between the leading edge of the right elevator and the right horizontal spar web access door in the aft part of the stabilizer. The restriction to elevator movement, caused by a highly unusual and unknown condition, was not detected by the crew in time to reject the takeoff successfully. However, an apparent lack of crew responsiveness to a highly unusual emergency situation, coupled with the captain's failure to monitor adequately the takeoff, contributed to the failure to reject the takeoff.
Source: NTSB-AAR-71-12, ¶2.2(b)
References
(Source material)
NTSB Aircraft Accident Report, AAR-71-12, Tran International Airlines Corp., Ferry Flight 863, Douglas DC-8-63CF, N486T, J. F. Kennedy International Airport, New York, Sept 8, 1970