These days, most airlines and flight departments preach the “no fault go around,” the idea that it is safer to go around when didn’t need to versus not going around when you should have. Way back in 1982, one of my Air Force squadrons used, “when in doubt, go around” as an instructor technique. There are countless accidents where a go around should have been called and wasn’t. What about times when a go around was called, but was ignored?
— James Albright
Updated:
2026-06-01
I think these happen more often than we like to admit, usually when the authority gradient is very steep. That is, when the captain is much senior in experience and flying time than the first officer. These captains usually get away with this breach in Crew Resource Management (CRM). But not always.
1 — Alitalia 404 in Zurich, Nov 14, 1990
2 — Air India Express Flight 812, 737, Mangalore, May 22, 2010
1
Alitalia 404 in Zurich, Nov 14, 1990
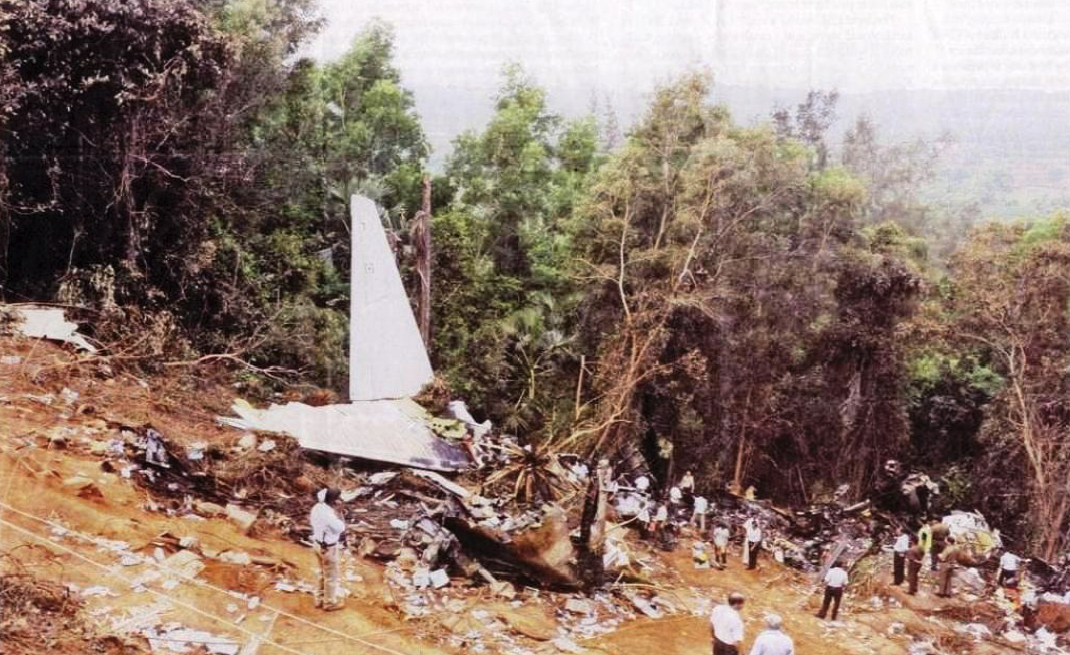
Alitalia Flight 404 departed Milan - Linate on November 14, 1990, bound for Zurich-Kloten, Switzerland. After a problem-free flight, the crew was cleared by Zurich Approach to descend to 4,000 feet and for the ILS 14 approach. The aircraft captured the localizer about 14 NM from the runway threshold and then flew through the cleared altitude. The descent rate was constant until impacting the ground about 5 NM from the runway. Everyone on board were killed and the aircraft was destroyed. [AAIB 1990/57, para. 0.1]
Date: November 14, 1990
Time: 2011 L
Type: Douglas DC-9-32
Operator: Alitalia
Registration: I-ATJA
Fatalities: 6 / 6 crew, 40 / 40 passengers
Aircraft Fate: Destroyed
Phase: Landing
Airport (arrival): Zurich-Kloten, Switzerland
The Crew
The captain was a 47-year-old Italian national with 10,193 total flying hours of which 3,194 were in type. He was a military veteran and had been flying for Alitalia for twenty years. He had been a captain for just over two years. [AAIB 1990/57, para. 1.5.1.1]
The copilot had much less experience by any metric. He was a 28-year-old Italian national with only 831 total flying hours of which 621 were in type. He was hired by Alitalia just sixteen months before the accident flight, presumably with only 200 hours total flying time. [AAIB 1990/57, para. 1.5.1.2]
This would be their second day on duty, having flown two legs the day prior followed by a 15 hour, 20 minute rest period. [AAIB 1990/57, para. 1.5.1.3]
Setup for failure
The VOR/ILS receivers.
The aircraft arrived on its previous flight with two Technical Logbook entries, one for VHF NAV 2 not displaying a To-FROM indication and the other for the autopilot failing to maintain glide path during a Cat II ILS. After the next flight, with the accident crew, the captain informed maintenance that the “failure had now been observed in position RADIO 1.” The maintenance team replaced both VHF-NAV receivers and asked the crew to fly a CAT II approach into Zurich so the aircraft could regain its CAT II status. [AAIB 1990/57, para. 1.0]
The aircraft ended up with a King model KNR6030 VOR/ILS receiver in the Number 1 position and a Collins 51RV-2B in the Number 2 position. There was a known issue with the KNR6030:
According to Douglas Aircraft Company engineers, it is possible that a short circuit or an open circuit in certain models of VOR/ILS receivers could cause navigation instruments to indicate “zero deviation.” Thus, raw data deviation information on the attitude direction indicator could center and remain centered with no failure or warning flag in view.
[NTSB ltr, A-92-8 and -9]
There is, however, a NAV instrument comparator that compares deviation signals of the glide path and localizer between the VOR/ILS receivers, but it only does this if the radio selector is set to the APP positions, when both NAV receivers deliver valid GP and LOC signals. In position RADIO 1 or RADIO 2, the comparator is not active. [AAIB 1990/57, para. 1.16.1.5.1]

[AAIB 1990/57, annex 8]

[AAIB 1990/57, annex 9]
With a mix of King and Collins VOR/ILS receivers, flying in the RADIO APP position would alert the pilots if the King receiver failed with zero deviation. Flying in the RADIO 1 or RADIO 2 position removes that protection.
Alitalia Standard Operating Procedure requires the APP position. [AAIB 1990/57, para. 1.16.1.11.1]
The altimeters.
Both altimeters were of the so-called, "Drum Pointer" type. These older models have the disadvantage that the altitude can only be read in two steps, because the main information is shown on the drum, and the refinements by a pointer on the round scale. A further complication is the fact that in certain pointer positions, the drum is not possible to read adequately as the numbers on the drum are partially obscured by the pointer. Despite the white band which appears on the left side of the "thousands" figures, this can lead to an incorrect interpretation of the "thousands" value.
[AAIB 1990/57, para. 1.16.2]
Headsets and microphones.
The quality of the CVR recording is bad. It required a great deal of work to understand the cockpit conversations recorded from the area microphone. The reasons for this bad comprehension is due on the one hand to the inferior technical quality of the recording equipment but in particular it is due to the fact that the pilots, even during the approach, did not make use of the headsets (with attached microphone) for communications with the approach Controller as is usual. The conversations between the pilots are therefore partly obscured by external radio traffic.
[AAIB 1990/57, para. 2.3.1.6]
The weather.
The weather into Zurich was mainly in cloud but during the descent became clear between 4,400 and 3,900 ft AMSL. Other aircraft had the approach and runway lighting “almost continuously in sight,” however this may not have been the case “for an aircraft flying too low.” [AAIB 1990/57, para. 1.7.1]
The approach
The first officer (COPI) was the pilot flying and the captain (PIC) was the pilot monitoring. The crew was cleared for the ILS 14 approach and to descend to 4,000 ft. [AAIB 1990/57, para. 1.7.1]
At 19:07:25, the crew selected RADIO APP. The captain’s GP indication was centered due to the King VOR/ILS receiver fault. The first officer’s ADI GP indication, in this mode, is slaved to the captain’s HSI and was also centered. The first officer’s HSI GP indication, however, correctly showed the aircraft well below glide path with a full-scale deflection. [AAIB 1990/57, para. 2.3]
At 19:07:40, the GP Comparator warning came on due to the disparity between GP indications. The first officer asked, “Do you have the glide?” The captain responded, “On one.” The first officer said, “I don’t have it.” [AAIB 1990/57, para. 2.3]
At 19:08:00, the captain said, “Good, let’s do it on one.” The first officer ordered the switch. Now both ADIs and both HSIs were using the faulty King VOR/ILS receiver and showed centered GP indications. The NAV selector was switched to ILS and GP-CAP was annunciated. The flight path changed from about 1,150 fpm descent rate to 700 fpm. [AAIB 1990/57, para. 2.3]
At 19:08:57, as the aircraft passed 3,700 ft., the altitude alert sounded because the selected altitude of 4,000 ft. was exceeded. The captain canceled the alert and changed the altitude select to 5,000 ft., the missed approach altitude. [AAIB 1990/57, para. 2.3]
At 19:10:43, the captain remarked that the DME showed 7 NM and said, “That doesn’t make sense to me.” His thoughts were interrupted by a radio call from Zurich Approach, instructing a switch to tower frequency. [AAIB 1990/57, para. 2.3]
At 19:10:59, the first officer called out, “Pull, pull, pull, pull,” and disconnected the autopilot. The first officer apparently correctly read his altimeter showing a height of 300 ft. QFE, causing him to commence a missed approach and order, “Go around.” The captain apparently misread his altimeter to read 1,300 ft. QFE. [AAIB 1990/57, para. 2.3]
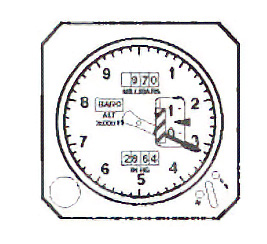
Depiction of altimeter at 19:10:59, (AAIB 1990/57, figure 12)
At 19:10:59 hrs, the beginning of the Go Around maneuver is clearly recognizable. Immediately (19:11:00 hrs) after the COPI’s “Go Around” order the PIC intervened as follows: “No, no, no, no . . . catch glide.”
[AAIB 1990/57, para. 2.3]

[AAIB 1990/57, figure 10, p. 141]
According to calculations from the investigating team and from the manufacturers the go around started by the Copilot 19 seconds before the accident would have been successful had it not been interrupted.
[AAIB 1990/57, para. 1.17.6]
At this point the DFDR shows a pitch change from -2° [AND] to +5.4° [ANU]. At the same time the thrust was increased from 1.3 to 1.7 EPR. The sink rate decreased from 1,100 ft/min. to 190 ft/min. After 11 seconds (the pitch oscillated at +1° [ANU]) the PIC asked "Can you hold it?" to which the COPI replied "Yes". One second after the COPI's answer the Radio Altimeter warning (pip pip pip) indicating 200 ft/AGL could be heard. During this, the PIC said "Hold on let's try to . . .” At 1911.18 hrs the aircraft struck the northern slope of the Stadlerberg at a altitude of 1,660 ft QNH.
[AAIB 1990/57, para. 1.1]
Standard Operating Procedures
From the evidence, there is no strict adherence to the ALITALIA procedures. Had the crew stuck to the procedures, the void between the PIC and the COPI, i.e. the coordination and cooperation, would probably have been covered at least in the critical phases. Extracts from the ALITALIA Company Manual (04.20.4/4):
Approach briefing
Initial Approach altitude
MSA (briefing)
Standard Operative Call-Outs “LOC alive”, “Glide alive”
Conditions requiring a missed approach
[AAIB 1990/57, para. 2.3.1.2]
Crew Resource Management
Investigators surmised that because “during the entire flight the conversation restricted itself to operational matters,” the PIC showed his “experience-based superiority.” [AAIB 1990/57, para. 2.3]
This may be what we today call a steep authority gradient.
Airmanship (Professional Competence.)
a) Crew
In general, it appears that during the flight the PIC's behavior was professional during routine operations. The impression does not apply when abnormal conditions appeared. In switching the Radio selector to RADIO 1, the crew did not proceed to an analysis of the cause of the (supposed) false indication, or even to make a subsequent crosscheck. It appears to have acted on a predetermined opinion (expected indication regarding the GP). The COPI continued the descent below the outer marker altitude although this had not been passed.
b) Crew as team
The teamwork in the critical phases was incomplete.
[AAIB 1990/57, para. 2.3.1.3]
About 40 seconds prior to impact, the first officer asked if the outer marker had been passed and the captain said that it had not. Then the captain noted that the DME didn’t make sense and a radio altimeter warning sounded ten seconds later. The first officer initiated the go around, but the captain overruled him. The first officer failed to challenge the captain’s decision. [AAIB 1990/57, para. 2.3.1.5]
Lessons Learned
There are several “micro” lessons from this crash, most of which could have been solved by the one “macro” lesson. First, the micro.
1. Know your aircraft’s limitations to include those of individual components. If the altimeter is easy to misread, learn to verbalize what you are seeing so you can subconsciously check yourself and to give your crew a chance to do the same. If a certain mode of the avionics can bite you, such as the RADIO APP mode in this aircraft, understand the risks and devise a mitigation strategy.
2. Adopt Standard Operating Procedures even if you have survived without them, realizing they are designed to protect you when circumstances, such as faulty equipment, conspire against you.
3. Fully brief stabilized approach criteria to include reasons to go around, agree that all it takes is either pilot to initiate the go around, and a go around call cannot be overruled.
The macro lesson is all about authority gradient; the lesson comes in two parts. First, for captains: understand that a wide gap in experience level puts the other pilot at a severe disadvantage that you, the captain, will have to address. A first officer who too easily agrees with your decisions or is reluctant to speak up robs you of a sanity check. No matter your experience level, you need that measure of quality control. Second, for first officers: realize that you will arrive at the scene of the accident the same time the captain does. If the captain makes a non-critical mistake, voice your opinion tactfully. If you think the mistake will be critical, then speak up tactfully at first, and then more forcefully as needed.
2
Air India Express Flight 812, 737, Mangalore, May 22, 2010
For the first 1 hour and 40 minutes of the Cockpit Voice Recorder (CVR), which recorded the last two hours of the flight, there was no conversation between the pilots because the captain was asleep and could be heard snoring. The flight was during the Window of Circadian Low (WOCL) but the crew did have the required rest period before the flight. Because a special qualification was needed to land on the “tabletop runway” at Mangalore, the captain would be required to carry out the landing. The crew didn’t plan the approach properly and was almost twice as high as the glide slope during the approach. The first officer made three go around calls, which the captain ignored. [Accident Report, pp. viii - ix]
The flight did not end well.
Air India Express 812, (Accident Report, cover)
Date: May 22, 2010
Time: 0605 India Standard Time (IST)
Type: Boeing 737-8HG
Operator: Air India Express
Registration: VT-AXV
Fatalities: 6 / 6 crew, 152 / 160 passengers
Aircraft Fate: Destroyed
Phase: Landing
Airport (arrival): Mangalore-Bajpe Airport (IXE), India
The Crew
The captain was a 55-year-old Serbian who got his start in erstwhile Yugoslavia and flew for JAT airline in that country until Yugoslavia was dissolved. He then flew in several other countries, including Malta, Canada, and Australia. He had 10,215 flight hours as a PIC, 2,844 in type. He was hired by Air India Express as a captain in 2008. He appeared to be friendly and well liked, except some of the first officers who had flown with him said he was “assertive in his actions and tended to indicate that he was ‘ALWAYS RIGHT.’” [Accident Report, para. 1.5.1]
The first officer was a 40-year-old Indian national with 3,620 total flight hours of which 3,320 were in type. He was due for upgrade to captain. He was known for being meticulous in his adherence to procedure and for being “a man of few words.” He had previously complained about another foreign national captain for not following company SOPs and having poor CRM techniques. [Accident Report, para. 1.5.2]
Setup for failure
Five months before the accident flight, the captain was counseled by the airline’s Chief of Flight Safety for a hard landing incident. The captain was said to be upset about the counseling because it was the first officer’s landing and it was just over the company’s “Vg” limit,1.9 Vg, but still below the manufacturer’s limit of 2.1 Vg. [Accident Report, para. 1.5.1]
The captain was suffering from an upset stomach and a sore throat prior to the accident. The report says, “it is possible that the captain was not fully fit on the day of the flight.” [Accident Report, para. 2.14.3]
The regularly scheduled flight was slated to depart Mangalore at 21:35 IST, land in Dubai at 02:45 IST, and to return to Mangalore at 06:30 IST. Much of the flight duty is during the WOCL. [Accident Report, para. 1.1]
The approach
The accident flight was through the WOCL and both pilots exhibited signs of being tired. The captain was audibly snoring, and the first officer could be heard yawning several times. They began their descent late and were much higher than would be expected throughout the DME Arc approach. The captain apparently realized this and selected the landing gear with the speed brakes still deployed at an altitude of 8,500 ft. [Accident Report, para. 1.1]
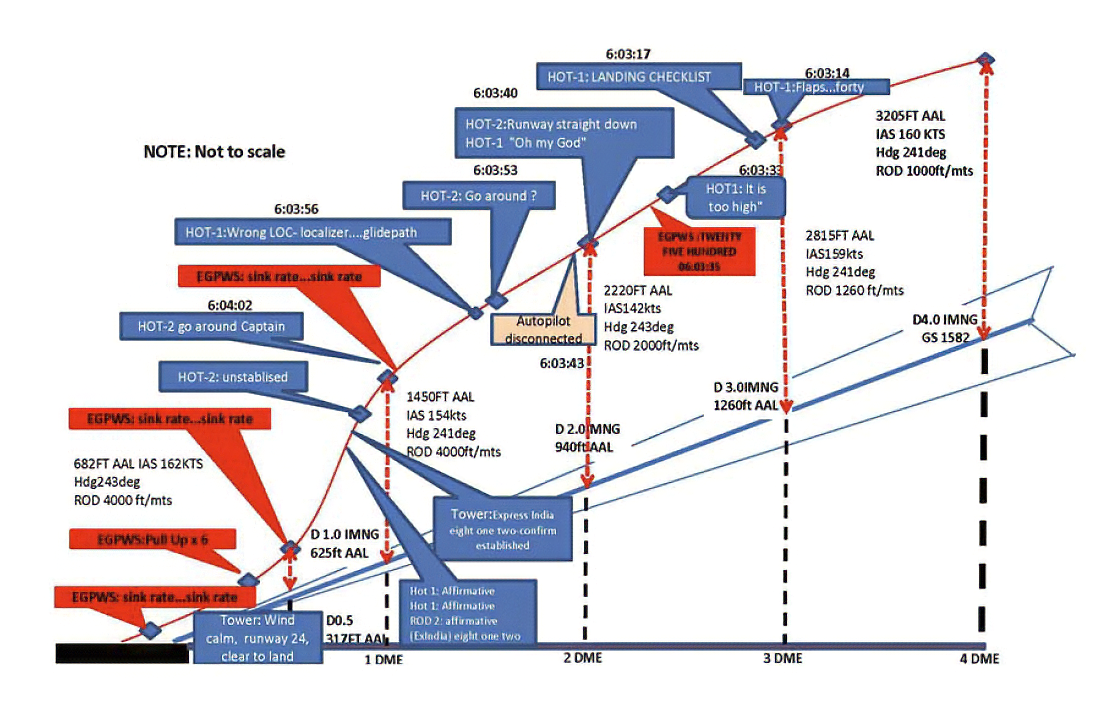
Approach profile including salient recordings from CVR (Accident Report, diagram 3)
During approach, the CVR indicated that the captain had selected Flaps 40° and completed the landing checklist. At 06:03:35 hours IST at about 2.5 DME, the radio altimeter had alerted an altitude of 2,500 ft. This was immediately followed by the first officer giving a call of “IT IS TOO HIGH” and “RUNWAY STRAIGHT DOWN.” In reply, the captain had exclaimed “OH MY GOD.” At this moment, the captain had disconnected the autopilot and simultaneously increased the rate of descent considerably to establish the desired approach path. At this stage, the first officer had queried “GO AROUND?”
To this query from the first officer, the captain had called out “WRONG LOC . . . LOCALISER . . . GLIDE PATH.”
[Accident Report, para. 1.1]
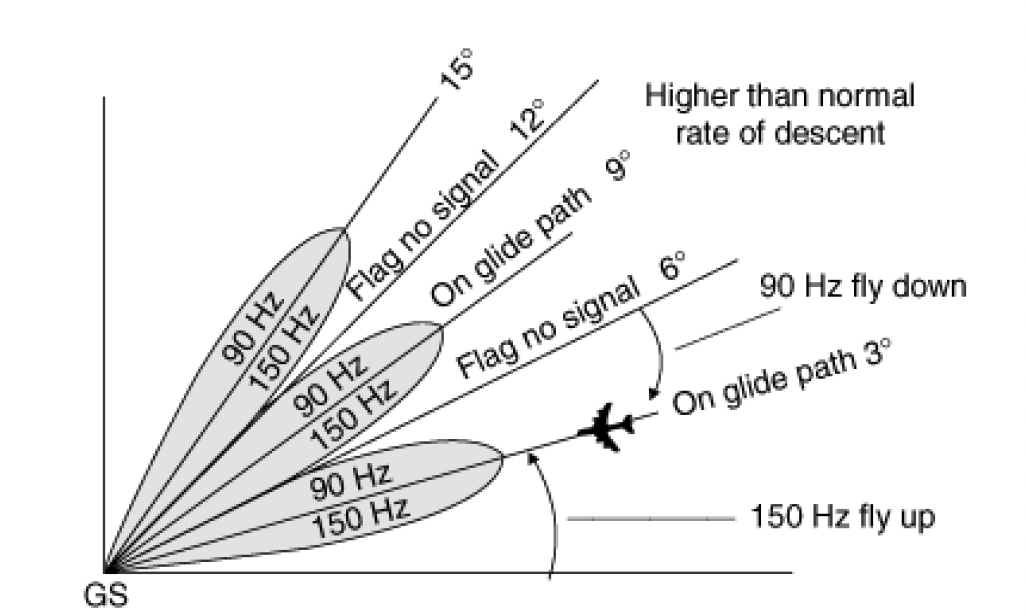
False ILS glide path, [Accident Report, diagram 16]
The radiation pattern of an ILS glide slope antenna can result in more than one overlapping lobe, usually in multiples of the true glide slope angle. (The exact angles depend on the frequency, antenna installation geometry, and terrain.) In some cases, the 90 and 150 Hz signals can invert, giving pilots reverse sensing. The solution to avoid these false glideslopes is to capture the proper glideslope from below. You should crosscheck your descent rate; if you are descending much faster than predicted, you may be on a false glideslope. In the report’s example, shown on diagram 16, a false glideslope exists at 9° and shows a centered glideslope indicator.
The first officer had given a second call to the captain for “GO AROUND” followed by “UNSTABILISED.” However, the first officer did not appear to take any action to initiate a go around. Having acquired the R/W visually and to execute a landing, it appears the captain had increased the rate of descent to almost 4,000 ft per minute. Due to this, there were numerous warnings from EGPWS for ‘SINK RATE’ and ‘PULL UP.’
[Accident Report, para. 1.1]
The aircraft’s airspeed was 142 kt. when the first officer said the runway was “straight down.” The captain pushed the nose over, causing the airspeed to increase. When the speed reached 162 kt., the Flaps Load Relief System (FLRS) automatically retracted the flaps from Flaps 40 to Flaps 30. [Accident Report, para. 2.2.14]
The tower asked if they were established on ILS approach, to which the captain prompted the first officer to answer “Affirmative.” The Flight Data Recorder showed they crossed the runway threshold at 200 feet with an indicated speed of 164 kt, 20 knots higher than the computed speed for their landing weight. [Accident Report, para. 2.2.14]
Short of touchdown, there was another (third) call from the first officer, this time on VHF channel “GO AROUND CAPTAIN” followed by “WE DON’T HAVE RUNWAY LEFT” on intercom.
[Accident Report, para. 1.1]
The FLRS later automatically extended the flaps when the speed slowed below 158 kt. This extension during the flare caused the aircraft to float. [Accident Report, para. 2.2.14]
The captain continued the landing, and the final touchdown was about 5,200 ft. from the threshold of Runway 24, leaving approximately 2,800 ft of remaining paved surface. [Accident Report, para. 1.1]
After having commenced braking, the captain made a grave mistake of stowing thrust reversers and opening full throttle with the intention of going around. The Boeing SOP categorically states that during landing, having selected thrust reversers, these should not be cancelled to initiate another takeoff. Despite such clear instructions, the captain had tried to go around. This further aggravated the situation and the aircraft impacted the non-frangible ILS mounting structure close to the airport fencing and fell into a gorge.
[Accident Report, para. 2.2.16]
The impact and subsequent fire destroyed the aircraft and killed all 6 crewmembers and 152 of 160 passengers. [Accident Report, para. 1.1]
Standard Operating Procedures
Air India Express had conventional stabilized approach rules, mandating the approach be stable by 1,000 feet altitude IFR and 500 feet if VFR. If the desired approach conditions were not met by these altitudes, the first officer was required to give a go around call, and the captain was required to do so. [Accident Report, para. 1.17.3.7]
Some of the pilots, who deposed in the Court had stated that a ‘Go Around’ had to be followed up by an Operational Incident Report (OIR). Many pilots felt that such reporting also added pressure on them while flying.
It was also given to understand by one of the foreign pilots that when he had to Go Around at one of the airports, the ATC controller had asked for the captain’s particulars and also the reason for going around. Such R/T call on an open channel was not only embarrassing for this pilot, but after landing, he was asked by the media.
[Accident Report, para. 1.17.3.8]
Crew Resource Management
Air India Express senior management say that CRM is covered during initial training and simulator LOFT exercises.
[Accident Report, para. 1.17.5.3]
The first officer did speak up three times, starting with a question, “Go around?” He followed this with a directive statement and finally by transmitting the go around call on the radio. But he did not take any action to prevent the captain from landing, such as assuming control of the aircraft. This begs two questions: why was the captain so reluctant to go around and why was the first officer reluctant to take action? I think a clue exists with the captain’s earlier hard landing counseling.
While the aircraft manufacturer specifies that 2.1 Vg, with other factors, correlates to a hard landing, the Air India Express Flight Safety Department set a limit of 1.65 Vg and used 1.8 Vg or more to determine when verbal counseling was to be used.
The flight crew, who had deposed in the Court, expressed their apprehension at being called to the Flight Safety Department for counseling, as it could well mean a blot on their career. A number of pilots had expressed such anxiety and possibility of stress while executing a landing to conform to these limits.
It is a common industry practice to call the flight crew for counseling in case of a serious violation of safety standards. However, each operator adopts different techniques to counsel the flight crew, with a purpose of correcting any wrong practice especially, if it is noticed to be a trend with such a pilot. Further, personal interaction allows an erring pilot to explain the circumstances, so that the incident can be analyzed more comprehensively. It also allows the supervisors to address shortcomings, if any, in the training being imparted.
The pilots of Air India Express, on the other hand, are averse to being called by the Flight Safety Department since it is considered that any adverse remarks would jeopardize their career progression. The pilots consider it somewhat demeaning and further stressful, if such counseling is indicated on Crew Schedules and is open information to other pilots.
[Accident Report, para. 1.17.6.2, 1.17.6.3]
As the report notes, these counseling sessions should be done with discretion, “so that a pilot does not feel embarrassed,” and “not to intimidate a pilot.” [Accident Report, para. 1.17.6.3]
Lessons Learned
As I started studying this accident, my first thought was the crew was set up by the schedule. But the pilots were given ample rest time prior to the WOCL flight. The captain had two nights off in a local hotel and the first officer lived in Mangalore and spent those nights at home. Flying early in the morning isn’t optimal, but it is the job.
I next wondered about the captain’s health. The captain’s family said he was suffering from an upset stomach and sore throat. The report says he may have been unfit to fly, and it is evident that the captain suffered from sleep inertia during the approach.
We cannot excuse the captain’s failure to plan and execute a stable approach or his failure to go around when the first officer called for it. We also cannot excuse the first officer’s failure to take the next step to prevent the crash by taking command of the aircraft. But we must also acknowledge that while these failures led to the accident, they were not the precipitating cause. I think it all began with airline management.
The report indicates an adversarial relationship between management and its pilots. The airline can say in writing that go arounds are required when approaches are unstable, but their actions requiring Operational Incident Reports following go arounds say otherwise. The report says the captain’s counseling over the earlier hard landing incident “cannot be considered as a contributing factor.” I disagree. The captain was indeed the reason this crash occurred. But I do think the airline’s pressure against go arounds was also a factor. It may also have been a factor pressuring the captain to fly when the wiser decision would have been to call in sick.
The technical lessons from this accident are fairly obvious and easy to learn. That isn’t true of the interpersonal lessons. First, the technical:
1) Brief the approach fully, including what it takes to descend into the approach environment, stable approach criteria, and the non-negotiable reasons to go around.
2) Monitor the descent in terms of track miles to go and target altitudes.
3) Intercept the glideslope from below, if possible, crosscheck the descent rate. A good rule of thumb for a descent rate on a 3° glide path is to take half your ground speed and add a zero. (120 kts groundspeed on a 3° glideslope should give you 600 ft/min.)
As for the interpersonal lessons:
1) When directing a go around, starting in a form of a question leaves open the possibility of a refusal. The go around call needs to be a command.
2) If the pilot flying refuses the go around call, transmitting the call on the radio is an excellent way to prompt the correct response.
3) When faced with a pilot who has “tunnel vision” or “target fixation” to salvage an unsalvageable landing, the next step becomes very hard to accomplish. If you feel certain the results will hurt the airplane and its occupants, you make the call “Go Around now or I’ve got the aircraft,” then execute the go around. I’ve never had to do this but have rehearsed the scenario in my head. My thought process includes: I’d rather be fired from the airline and live, than honored by the airline posthumously for being a team player.
4) When in doubt and you have the fuel to go around, then go around. If the airline makes you report that, do so. If the airline counsels you verbally or in writing, so be it. Once again: I’d rather be fired from the airline and live, than honored by the airline for having died on duty.
5) If the airline publicizes the fact you’ve been chastised, approach the guilty parties privately. If they persist, seek union protection. If that fails, seek another employer.
3
Cessna 560XL, N46CF, 2021
If you ever find yourself crossing the runway threshold with an extra 50 knots, it might be a little late to think, “I can salvage this approach.” That was this captain’s thought, even after the first officer called for a go around four times. The captain’s response? “No, we are landing.”

N46CF in the EMAS, NTSB Docket Photo 2
Date: July 21, 2021
Time: 1604 L
Type: Cessna 560XL
Operator: PV Transport Inc
Registration: N46CF
Fatalities: 0 / 2 crew, 0 / 4 passengers
Aircraft Fate: Substantially damaged
Phase: Landing
Airport (arrival): Reading Regional Airport / Spaatz Field, PA (KRDG)
The NTSB couldn’t be bothered to visit the accident site and devoted a scant six pages to the final report. I guess you can’t blame them: nobody was injured, except the airplane. As for the airplane, a 20-year-old Citation XL wasn’t worth much more than $ 2 million at the time. So, there aren’t a lot of details available and the most important point was left out by the investigators entirely. But more on that later.
The Crew
The captain was 49 years old at the time and had 5,412 total flight hours of which 412 were in type. He had type ratings in the LR-JET, G-200, CE-560XL, and MD-11. [ERA21LA296 docket]
The first officer was 24 years old at the time and had 1,929 total flight hours of which 396 were in type. He had type ratings in the BE-300 and CE-560XL, as well as an SIC type in the CE-500. [ERA21LA296 docket]
Setup for failure
The conditions were ideal: day, 10 miles visibility, few clouds at 1,800 feet, light winds, dry runway. [ERA21LA296 Final Report]
Reading “between the lines,” however, there was a potential for problems. The captain had more than double the first officer’s experience in terms of age and flight hours. The first officer did speak up during the approach but didn’t follow through.
The approach
We were cleared to land Runway 13 at KRDG.
The PIC was flying.
On a 5-mile right base, I reported that we appeared high.
On 3-mile final, I reported “high and fast.”
At 3 nm from the threshold, the aircraft GPROX system called “Terrain, Pull Up.” I responded to GPROX call with “Go Around,” followed by no answer from the PIC.
On 2-mile final gear was selected down.
Still being high and fast I called “Go Around” again at 1 mile final.
The speed was estimated at 160 knots.
Over the threshold I stated, “Go Around” then something along the lines of “put this thing down” followed by “Go Around” this was the first call the PIC responded to and said “No, we are landing.”
[First Officer’s Email Statement ERA21LA296 docket]
Standard Operating Procedures
The accident docket includes an excerpt from Image Air LLC Standard Operating Procedures, so we can assume the crew had SOPs, but we don’t know how well they were trained or checked.
Crew Resource Management
In a conversation with the captain, the investigator noted the captain “takes responsibility for the breakdown in CRM.”
The PF stated immediately, that he “took a perfectly good first officer and ignored him.”
He became “target fixated.”
And wanted to land the airplane, thinking that he could salvage the approach and land safely.
During final, he thought he would be able to slow it sufficiently, but it was evident that during the landing, they were carrying too much speed and by that point, they were committed because the airplane was fully configured for landing. They were “eating up a lot of runway” before finally settling onto the pavement. They added full brakes and deployed the reversers but rolled into the EMAS system.
[Contacted: Pilot Flying, ERA21LA296]
It’s easy enough to “be trained” in CRM, but it is incumbent on those being trained to take the lessons to heart. If the environment doesn’t allow feedback, a pilot with a blindness to CRM will never know. About that . . .
The PM felt like he was “just a passenger” during the initial approach. He felt like, short of wrestling the controls away from the pilot, there was nothing else he could do. He challenged the PF multiple times during the approach without results.
[Contacted: Pilot Monitoring, ERA21LA296]
Another EMAS Save
What the report leaves out . . .

Terrain drop at KRDG, Runway 13 departure end (GoogleEarth)
As far as I can tell after plotting the Runway 13 extended centerline, the terrain drops about 400 feet after the EMAS, ending 90 feet lower at the Schuylkill River. (The river name comes from early Dutch settlers and means “hidden river.”)
I think that without the EMAS, the outcome would have been tragic. The two pilots and four passengers are lucky to be alive.
Lessons Learned
There are obvious lessons in this accident but stating the obvious will be of no use to those who need the lessons the most. The worst part of that is that those who need the lessons the most are the least likely to realize that. So, let’s address this as if we are talking to all pilots, even those who are certain they would never make the same mistakes.
As the Pilot Flying: the only way you can benefit from the safety of a stable approach is to take every approach seriously. Evaluate your progress:
- At the final approach fix or glide slope intercept during an instrument approach
- At 1,000 feet on a visual straight-in
- On base-to-final during a circling approach
If you don’t have the numbers “wired” by these points, verbalize the disparities and announce you will go around if you don’t have them solved by 500 feet VMC / 1,000 feet IMC. This becomes a promise to the Pilot Monitoring. And then follow through.
As the PM: your integrity is on the line as much as the PF’s. Becoming “just a passenger,” as the accident first officer stated, is a cop out. There are graduated responses to an unresponsive PF:
- Announce the problems without the phrase “Go Around” to give the PF the chance to make the call.
- Make the go around call authoritatively, not as a suggestion. “Unstable, go around.”
- If you have time for a second attempt, include a threat, “If you don’t go around, I will take control of the aircraft and execute the go around myself.”
- If the PF continues, toggle TO/GA, push the throttles forward, say, “I’ve got it.”
If you are thinking that last bit was a bridge too far, consider in our earlier case studies the PMs died while “just a passenger.” In the case of this accident, the first officer’s hope for a successful career must surely be over. I would never hire him.
4
United Express 4339, 2025
In another case of becoming fixated on landing and being saved by the EMAS, this United Express landed in heavy rain and failed to stop in the confines of the runway. The crew computed that with a Runway Condition Code of 5, (less than 1/8-inch depth of water), they would have a margin of only 200 feet. When it became apparent they had a problem, the first officer called for a go around twice. The captain continued and the results were predictable.

Aircraft in the EMAS, NTSB DCA25LA339, Figure 2.
Date: September 24, 2025
Time: 2117 L
Type: Embraer EMB-145XR
Operator: CommuteAir (dba United Express)
Registration: N21129
Fatalities: 0 / 3 crew, 0 / 50 passengers
Aircraft Fate: Minor damage
Phase: Landing
Airport (arrival): Roanoke-Blacksburg Regional Airport (KROA), Roanoke, VA
The final report is still pending and as of this writing, the NTSB docket isn’t available. So, all of what follows is from the preliminary report. I offer it only as the most recent example to illustrate that the ignored go around call is still with us.
The Crew
The captain was the Pilot Flying and the first officer was the Pilot Monitoring.
Setup for failure
It was a night flight with the weather forecast of clouds at 3,200 ft. AGL, a ceiling at 4,900 ft. AGL, 1.75 miles visibility. En route, the ATIS reported calm winds, no precipitation, a cloud ceiling of 15,000 ft., and that Runway 6 was in use. The first officer suggested reviewing landing performance for a wet runway, but the captain declined because of the ATIS report. Checking in with approach control, they were informed about precipitation along the approach path to Runway 6 and that other aircraft were using Runway 34. The crew set up for an ILS to Runway 34. [Preliminary Report, DCA25LA339, p. 1]
The approach
After turning on final approach, the flight crew observed the runway and heard the previous landing aircraft report marginal visibility and bumpy conditions. During the approach, the rain intensity increased, and the captain requested that the FO run the performance calculation for landing on a wet runway with a RCC of 5. The FO ran the performance calculations and determined that they would have a margin of approximately 200 feet more than was required, without thrust reverser usage. The captain briefed the go-around procedures and that they would divert to Piedmont Triad International Airport (GSO), Greensboro, North Carolina if they executed a go-around.
On short final, the rain intensity increased, and the captain requested windshield wipers at high. As the airplane descended below 500 feet, the FO observed that they were high on the precision approach path indicator (PAPI) and then observed the captain correcting the flight path, but recalled they were still high as the airplane crossed the threshold. After crossing the runway markings, the FO called for a go-around, but the captain continued. About halfway down the runway, the FO called for a go-around a second time, but the captain continued.
The airplane touched down and the flight crew applied maximum braking and deployed the engine thrust reversers. The airplane overran the end of the runway and came to rest in the EMAS.
[Preliminary Report, DCA25LA339, pp. 2 - 3]
Lessons Learned
I will not speculate about problems with CRM or SOPs and will wait for the final report to be issued. The lessons of the previous three case studies, however, apply.
Way back in 1990, perhaps before these two pilots were even alive, the crew of Alitalia learned that following SOPs can be critical when the unexpected happens.
Twenty years later, the captain of Air India Express 812 refused the first officer’s go around calls until it was too late. The first officer verbalized the go around but failed to intervene when it became obvious failing to do so would be a fatal mistake.
Five years ago, the crew of a business jet was lucky to survive because the runway’s EMAS prevented them from careening down a hill into a river. The first officer said he felt like a passenger and that was apt, he essentially became a passenger when the captain refused to go around.
The obvious lessons you will read from these accident reports is that captains need to go around when the first officer calls for it. But nowhere will you find what needs to happen after the captain refuses to go around. If the alternative is probable loss of life, the answer is to toggle TO/GA, push the throttles forward, and say, “I have control of the aircraft.”
References
(Source material)
Aviation Investigation Final Report, Accident Number ERA21LA296, Cessna 560XL, N46CF, Reading, PA, July 21, 2021, 1604 Local.
Aviation Investigation Preliminary Report, DCA25LA339, Embraer EMB-145XR, N21129, Roanoke, VA, September 24, 2025.
Final Report of the Federal Aircraft Accidents Inquiry Board (AAIB) concerning the Accident of the aircraft DC-9-32, ALITALIA, Flight No AZ 404, I-ATJA on the Stadlerberg, Weiach/ZH, of November 1990, Nr. 1990/57 (Translation of the German original context).
National Transportation Safety Board (NTSB) Safety Recommendation, February 4, 1992, Refer to A-92-8 and -9.
Report on Accident to Air India Express Boeing 737-800 Aircraft VT-AXV on 22nd May 2010 at Mangalore, Government of India Ministry of Civil Aviation, New Delhi, 31st October 2010